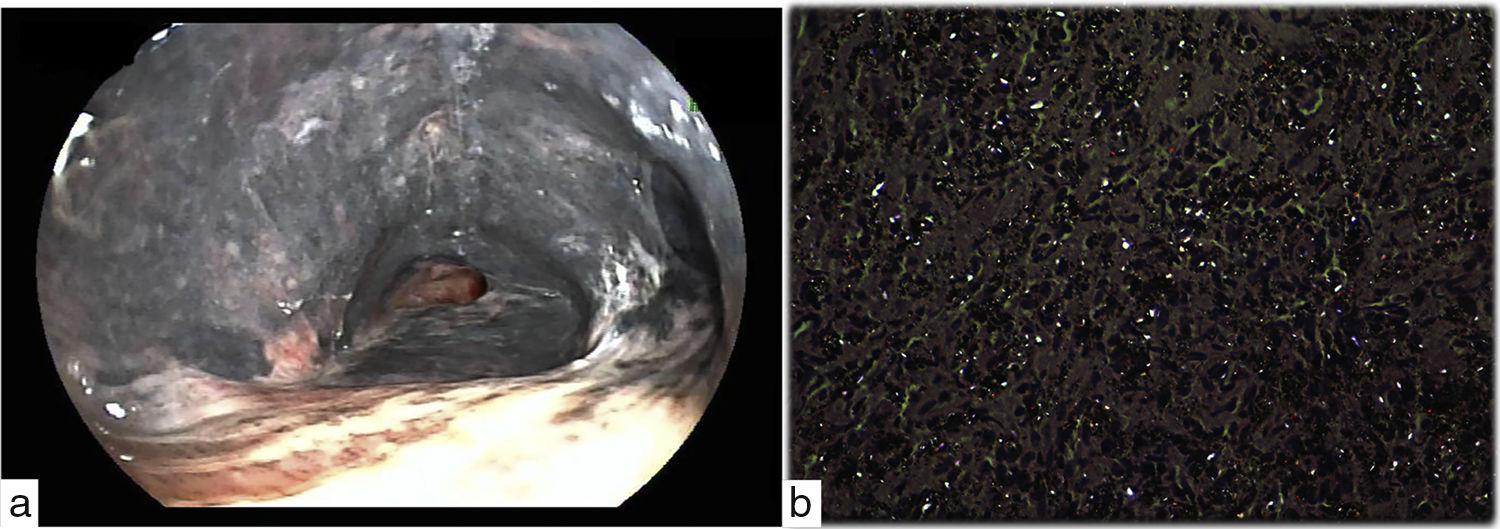
A 68-year-old man referred to pulmonary consult with a 6-month history of increase shortness of breath and dry cough. He has worked in a copper mine north of Chile for almost 40 years. On physical examination, breath sounds were reduced bilaterally along with mild crackles. Laboratory studies revealed erythrocytosis with hematocrit 54% and hemoglobin 18.5g per deciliter (reference range, 13.5–17.5). Chest-CT scan showed mass-like lesions and bronchial narrowing in both upper lobes. Flexible bronchoscopy demonstrated mucosa dark pigmentation from both main stem bronchi and bronchus intermedius together with segmental bronchi obliteration of both upper lobes (Fig. 1A and Video). Bronchial mucosa biopsy revealed coal dust and acicular crystalline material observed under polarized light (40×) (Fig. 1B). Anthracofibrosis results from carbon particles deposition but other organic and inorganic substances,1,2 like silica in this case, can also cause this pigmentation.2 Commonly reported radiological features includes central peribronchial soft tissue thickening, intraparenchymal peribronchial cuffing or bronchial narrowing, such our case.1 Definitive diagnosis included a bronchoscopic examination that revealed a dark pigmentation in airway and biopsy samples revealed infiltration of non-specific mononuclear inflammatory cells, mostly polymorphonuclears with a normal epithelium.2 Unfortunately, there is no treatment for this condition rather than avoid exposure.
Impact factor
The Impact Factor measures the average number of citations received in a particular year by papers published in the journal during the two preceding years.
© Clarivate Analytics, Journal Citation Reports 2025
Impact factor 2024
9.2
Citescore 2024
3.5
SJR
SRJ is a prestige metric based on the idea that not all citations are the same. SJR uses a similar algorithm as the Google page rank; it provides a quantitative and qualitative measure of the journal's impact.
See moreSJR 2024
0.466
SNIP
SNIP measures contextual citation impact by wighting citations based on the total number of citations in a subject field.
See moreSNIP 2024
0.505
View more metrics