
Peripheral neuropathy (PN) is a disease that affects the peripheral nerves due to any number of causes (hereditary, infectious, toxic, etc.). It may be classified according to the number of nerves that are affected, as mono or polyneuropathy, and according to the affectation of the nerve structure, as demyelinating, axonal or mixed.1
We present an 80-year-old patient, who has been an ex-smoker for the last 30 years, with an accumulated tobacco consumption of 70 pack-years. The subject had been diagnosed with chronic obstructive pulmonary disease (COPD) with severe airflow obstruction (post-bronchodilator forced expiratory volume in 1s [FEV1] of 40%) and had been treated with long-term home oxygen therapy at 2l/min, 24h/day (PaO2 in stable phase 64mmHg with oxygen and 46mmHg without) for more than 10 years. The last COPD exacerbation was in 2010.
The patient came to our pulmonology consultation for a scheduled visit in May 2011. During this visit, he reported having a burning chest pain which made it difficult to breathe. The pain was daily and continuous, although it improved when lying down, and became more intense in the evening. The patient also complained of a tickling sensation in both feet and in the right thigh, with numbness of the internal dorsum of the left foot. Given the clinical suspicion for PN, an EMG was ordered, which revealed normal nerve conduction velocity with decreased nerve amplitude and with no positive sharp waves in either leg. The patient was sent to the neurology consultation for a complete study.
During follow-up, the patient presented neuropathic pain in both legs, and treatment was initiated with Hidroxil B1,B6,B12 and pregabalin at an increasing dosage until reaching 300mg/day, with poor pain control. This therapy was therefore substituted with carbamazepine, which provided better control of the symptoms, although the patient currently continues to have paresthesia in the legs and occasional pain.
The actual prevalence of PN in COPD is currently unknown, although there are several studies that indicate a frequent affectation of the peripheral nervous system, which on most occasions is subclinical.2
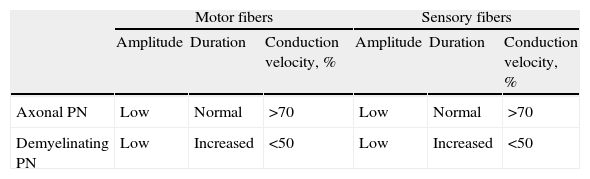
In the physiopathology of PN in COPD, several factors have been implicated. Although for the moment we do not precisely understand its contributing role, hypoxemia could be the main factor in the development of this type of PN.3 The neurophysiological characteristics are compatible with an axonal polyneuropathy with predominantly motor involvement4 (Table 1) and greater affectation of the legs, although it may involve any region.3
Electromyographic Characteristics of Peripheral Neuropathies (PN).
| Motor fibers | Sensory fibers | |||||
| Amplitude | Duration | Conduction velocity, % | Amplitude | Duration | Conduction velocity, % | |
| Axonal PN | Low | Normal | >70 | Low | Normal | >70 |
| Demyelinating PN | Low | Increased | <50 | Low | Increased | <50 |
In conclusion, PN seems to be a relatively frequent affectation in patients with COPD, especially in more hypoxemic patients who are treated with home oxygen, as in the case of our patient. Although the affectation is usually subclinical, we should be alert to the appearance of compatible symptoms in order to reach a correct diagnosis and initiate early treatment of symptoms.
Please cite this article as: Segrelles Calvo G, et al. Polineuropatía periférica en un paciente con enfermedad pulmonar obstructiva crónica grave. Arch Bronconeumol. 2012;48:484.







