
It has been well documented that metabolic alkalosis (MAlk) is a very frequent disorder that is usually associated with situations of chronic respiratory acidosis (RA). This should be of no surprise if we keep in mind the regularity with which these patients receive treatment with loop diuretics, thiazides or low-salt diets, which are common causes for this disorder. Nevertheless, the recognition of this association is very infrequent, despite the severe consequences derived from the increased hypoventilation entailed in the compensatory response of MAlk.1–3 Thus, in daily practice we repeatedly observe a tendency to automatically attribute any elevation in plasma bicarbonate to the compensatory mechanism of RA, regardless of the amount.
It has been perfectly established, on the other hand, that for the correct diagnosis of an acid–base disorder, it is necessary to have, in addition to the understanding of the patients symptoms and the filiation of the primary acid–base disorder, the detailed analysis of the compensatory mechanisms in order to estimate its coherence. In chronic RA, for example, increases in bicarbonate of 3.5mmol/l are considered normal for every 10mmHg that PaCO2 increases.4 Therefore, any deviation either above or below predicted would indicate the coexistence of alkalosis—which aggravates hypoventilation—or of metabolic acidosis (MA).
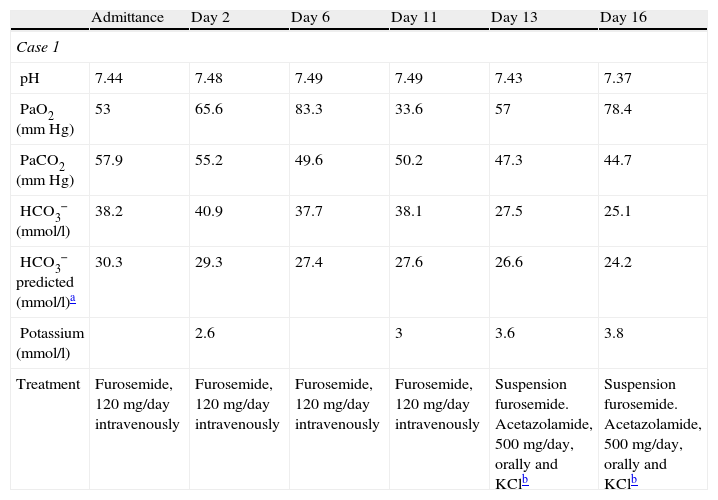
To illustrate this, we feel it is interesting to report two cases of chronic RA coexisting with MAlk that we have treated recently and which reflect the worrisome reality of a much larger universe. The first patient presented with obesity-hypoventilation syndrome, and the second with chronic obstructive pulmonary disease (COPD), both with cor pulmonale in addition. The lack of recognition of the mixed disorder caused worsened symptoms and poorer blood gas analyses in the two cases. In both instances, treatment with 500mg/day of acetazolamide (ACZ) for some days and the suspension of furosemide (the only relevant therapeutic modification) notably improved the situation. One of the patients was able to stop home oxygen therapy, which had been prescribed some months earlier (Table 1).
Evolution of Patient Blood Gases.
| Admittance | Day 2 | Day 6 | Day 11 | Day 13 | Day 16 | |
| Case 1 | ||||||
| pH | 7.44 | 7.48 | 7.49 | 7.49 | 7.43 | 7.37 |
| PaO2 (mmHg) | 53 | 65.6 | 83.3 | 33.6 | 57 | 78.4 |
| PaCO2 (mmHg) | 57.9 | 55.2 | 49.6 | 50.2 | 47.3 | 44.7 |
| HCO3− (mmol/l) | 38.2 | 40.9 | 37.7 | 38.1 | 27.5 | 25.1 |
| HCO3− predicted (mmol/l)a | 30.3 | 29.3 | 27.4 | 27.6 | 26.6 | 24.2 |
| Potassium (mmol/l) | 2.6 | 3 | 3.6 | 3.8 | ||
| Treatment | Furosemide, 120mg/day intravenously | Furosemide, 120mg/day intravenously | Furosemide, 120mg/day intravenously | Furosemide, 120mg/day intravenously | Suspension furosemide. Acetazolamide, 500mg/day, orally and KClb | Suspension furosemide. Acetazolamide, 500mg/day, orally and KClb |
| 1st Consultation | Day 30 | Day 45 | Day 48 | Day 52 | |
| Case 2 | |||||
| pH | 7.49 | 7.5 | 7.46 | 7.40 | 7.41 |
| PaO2 (mmHg) | 50.20 | 58.70 | 44.50 | 67.30 | 65 |
| PaCO2 (mmHg) | 47 | 51.60 | 63.10 | 43 | 42.4 |
| HCO3− (mmol/l) | 35 | 37.80 | 44.20 | 26.70 | 25.4 |
| HCO3− predicted (mmol/l)a | 26.4 | 28.10 | 32.10 | 24.10 | 24.5 |
| Potassium (mmol/l) | 2.9 | 3.3 | 3 | 3.7 | 4.1 |
| Treatment | Furosemide 60mg/day, orally | Furosemide 60mg/day, orally | Furosemide 60mg/day, orally | Suspension furosemide. Acetazolamide, 500mg/day, orally | Suspension furosemide. Acetazolamide, 500mg/day, orally |
Normal values. Arterial blood: pH: 7.36–7.44; PaCO2: 36–44mmHg; HCO3−: 22–26mequiv./l. Venous blood: pH: 7.31–7.37; PaCO2: 42–50mmHg; HCO3−: 23–27mequiv./l.
MAlk generally initiates with digestive loss (vomiting, nasogastric aspiration) or renal loss (diuretics) of hydrons (H+). As the hydrons come from the dissociation of H2CO3, for each mequiv. of H+ lost, another mequiv. of bicarbonate is generated. Given that the renal capacity for excreting the excess of bicarbonate is great, MAlk only perpetuates when certain circumstances coexist, such as a reduction in effective volemia, hypochloremia, hypokalemia or hyperaldosteronism, in which the renal reabsorption of bicarbonate is higher. The increase in plasma bicarbonate raises the pH, whose compensatory mechanism is hypoventilation that reduces PaO2 and increases PaCO2, which in turn compromises even more the respiratory situation in a patient with RA. The usual treatment used in MAlk (sodium chloride, potassium chloride, suspension of diuretics, etc.) may not be prudent in patients with chronic RA, especially if they present with edemas. It is in this context when ACZ is especially effective when used for some days. It is a mild diuretic that increases renal excretion of bicarbonate by the inhibition of carbonic anhydrase that, over the long-term, may cause AM. ACZ has already demonstrated its usefulness in hypercapnic respiratory failure in patients with COPD or with obesity-hypoventilation syndrome, even when there is no accompanying MAlk.5,6 It is, however, especially useful when said association is given, just as the clinical and blood gas evolution of our patients seems to endorse.
In short, we can affirm that MAlk frequently complicates and perpetuates situations of RA. Thus, we believe it necessary for the clinical services that are involved to analyze this problem and to implement pertinent actions. Lastly, it would be important to initiate controlled, randomized studies in order to more closely define the effectiveness of ACZ in this situation.
Please cite this article as: Prieto de Paula JM, et al. Sobre la importancia de identificar la asociación de alcalosis metabólica con acidosis respiratoria. Arch Bronconeumol. 2011;48:65–6.







