

These are times of transition in which healthcare delivery is capturing more attention and is clearly beginning to take an important position in patient care. The desire to improve patient safety has led to a series of initiatives aimed at implementing standard practices to improve quality in healthcare.1 Quality indicators are standardized measures for determining the appearance and intensity of a phenomenon or event.2 Intensive care units are not exempt from the application of an organizational model that can be measured from different angles and improved once areas of opportunity have been identified. One of the most important advances in the development of evidence-based quality indicators in intensive care has been made by the Spanish Society of Intensive and Critical Care Medicine and Coronary Units (SEMICYUC), together with the Avedis Donabedian Foundation.2,3 SEMICYUC generated quality indicators that were adopted by intensive care units in Spain and by other international scientific societies, such as the European Society of Intensive Care Medicine and the Indian Society of Critical Care Medicine. The proposals included not only general indicators, but also quality of care indicators for specific patient populations, such as coronary artery patients, who are often treated in dedicated units. Specialized units catering for patients with particular characteristics require specifically adapted indicators and standards, some of which may have to be more rigid than others.4
The aim of this project is to draw up recommendations for monitoring quality in units that, due to the type of patient they specialize in, share common features and are termed collectively “respiratory intensive care units”. The initiative was launched by the heads of the intensive care units in the chest clinics of tertiary and fourth-level hospitals in Mexico, namely (1) the Respiratory Intensive Care Unit of the Pulmonology and Thoracic Surgery of the Hospital General de México, (2) the Intensive Care Unit of the Instituto Nacional de Enfermedades Respiratorias (INER); (3) the Respiratory Intensive Care Unit of the Centro Médico Nacional “La Raza”, and (4) the Intensive Care Unit of the Department of Pulmonology and Intensive Care of the Hospital Universitario de Monterrey.
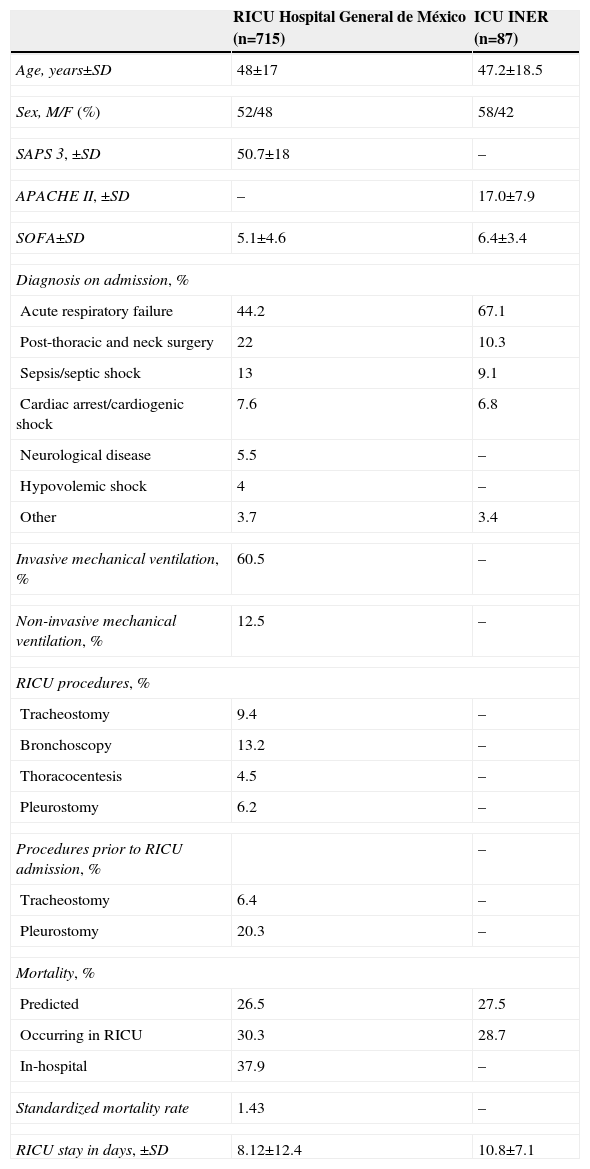
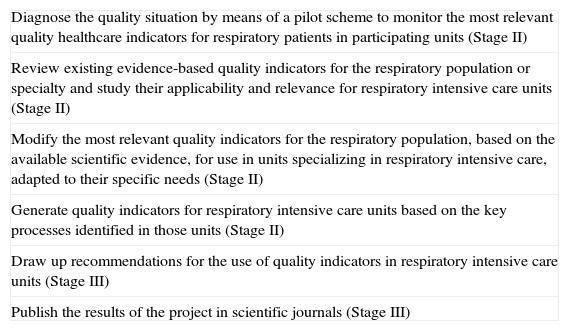
The first meeting of Task Force members took place during the 39th Annual Meeting of the Mexican Association of Critical Medicine and Intensive Care in León, Guanajuato in October 2012. At the meeting, the initial general objectives were defined, as follows: (a) to specify the features defining a respiratory intensive care unit (RICU) in Mexico, and (b) to characterize the type of patients seen in these units and define their needs. In a second meeting in March 2013, an RICU was defined as an intensive care unit that treats critical patients with predominantly respiratory diseases, placing emphasis on distinguishing this term from that used in previous publications from other countries referring to intermediate and/or chronic care units for the withdrawal of mechanical ventilation.5 Available statistical data were considered deficient (Table 1) and the team agreed to complete the first stage of the project by collecting relevant information from a prospective cohort. Specific project objectives that will be addressed in 2 subsequent stages are described in Table 2 and Fig. 1.
Available Statistics From 2 of the Participating Units.a
| RICU Hospital General de México (n=715) | ICU INER (n=87) | |
|---|---|---|
| Age, years±SD | 48±17 | 47.2±18.5 |
| Sex, M/F (%) | 52/48 | 58/42 |
| SAPS 3, ±SD | 50.7±18 | – |
| APACHE II, ±SD | – | 17.0±7.9 |
| SOFA±SD | 5.1±4.6 | 6.4±3.4 |
| Diagnosis on admission, % | ||
| Acute respiratory failure | 44.2 | 67.1 |
| Post-thoracic and neck surgery | 22 | 10.3 |
| Sepsis/septic shock | 13 | 9.1 |
| Cardiac arrest/cardiogenic shock | 7.6 | 6.8 |
| Neurological disease | 5.5 | – |
| Hypovolemic shock | 4 | – |
| Other | 3.7 | 3.4 |
| Invasive mechanical ventilation, % | 60.5 | – |
| Non-invasive mechanical ventilation, % | 12.5 | – |
| RICU procedures, % | ||
| Tracheostomy | 9.4 | – |
| Bronchoscopy | 13.2 | – |
| Thoracocentesis | 4.5 | – |
| Pleurostomy | 6.2 | – |
| Procedures prior to RICU admission, % | – | |
| Tracheostomy | 6.4 | – |
| Pleurostomy | 20.3 | – |
| Mortality, % | ||
| Predicted | 26.5 | 27.5 |
| Occurring in RICU | 30.3 | 28.7 |
| In-hospital | 37.9 | – |
| Standardized mortality rate | 1.43 | – |
| RICU stay in days, ±SD | 8.12±12.4 | 10.8±7.1 |
APACHE II: Acute Physiology and Chronic Health Evaluation II; SD: standard deviation; INER: National Institute of Respiratory Diseases; M/F: men/women; SAPS 3: Simplified Acute Physiology Score 3; SOFA: Sequential Organ Failure Assessment; RICU: respiratory intensive care unit.
Objectives.
| Diagnose the quality situation by means of a pilot scheme to monitor the most relevant quality healthcare indicators for respiratory patients in participating units (Stage II) |
| Review existing evidence-based quality indicators for the respiratory population or specialty and study their applicability and relevance for respiratory intensive care units (Stage II) |
| Modify the most relevant quality indicators for the respiratory population, based on the available scientific evidence, for use in units specializing in respiratory intensive care, adapted to their specific needs (Stage II) |
| Generate quality indicators for respiratory intensive care units based on the key processes identified in those units (Stage II) |
| Draw up recommendations for the use of quality indicators in respiratory intensive care units (Stage III) |
| Publish the results of the project in scientific journals (Stage III) |

The Task Force is currently receiving support from their respective hospitals (the most important tertiary and fourth-level centers in the Mexican health system), as well as the backing of the Mexican Pulmonology Council. In the future, we hope to gain the support of the Mexican College of Critical Medicine, the Mexican Society of Pulmonology and Thoracic Surgery and other scientific societies, with the aim of achieving the widespread dissemination of acceptable results.
Please cite this article as: Álvarez-Maldonado P, Bautista-Bautista E, Huizar-Hernández V, Mercado-Longoria R, Cueto-Robledo G. Grupo de trabajo para la revisión, modificación y desarrollo de indicadores de calidad para unidades de cuidados intensivos respiratorios en México. Arch Bronconeumol. 2015;51:357–358.







