



Pregnancy is associated with certain specific physiological adaptations and some atypical symptoms can be misdiagnosed during this period, leading to serious complications, particularly if pregnancy is associated with tumor disease.
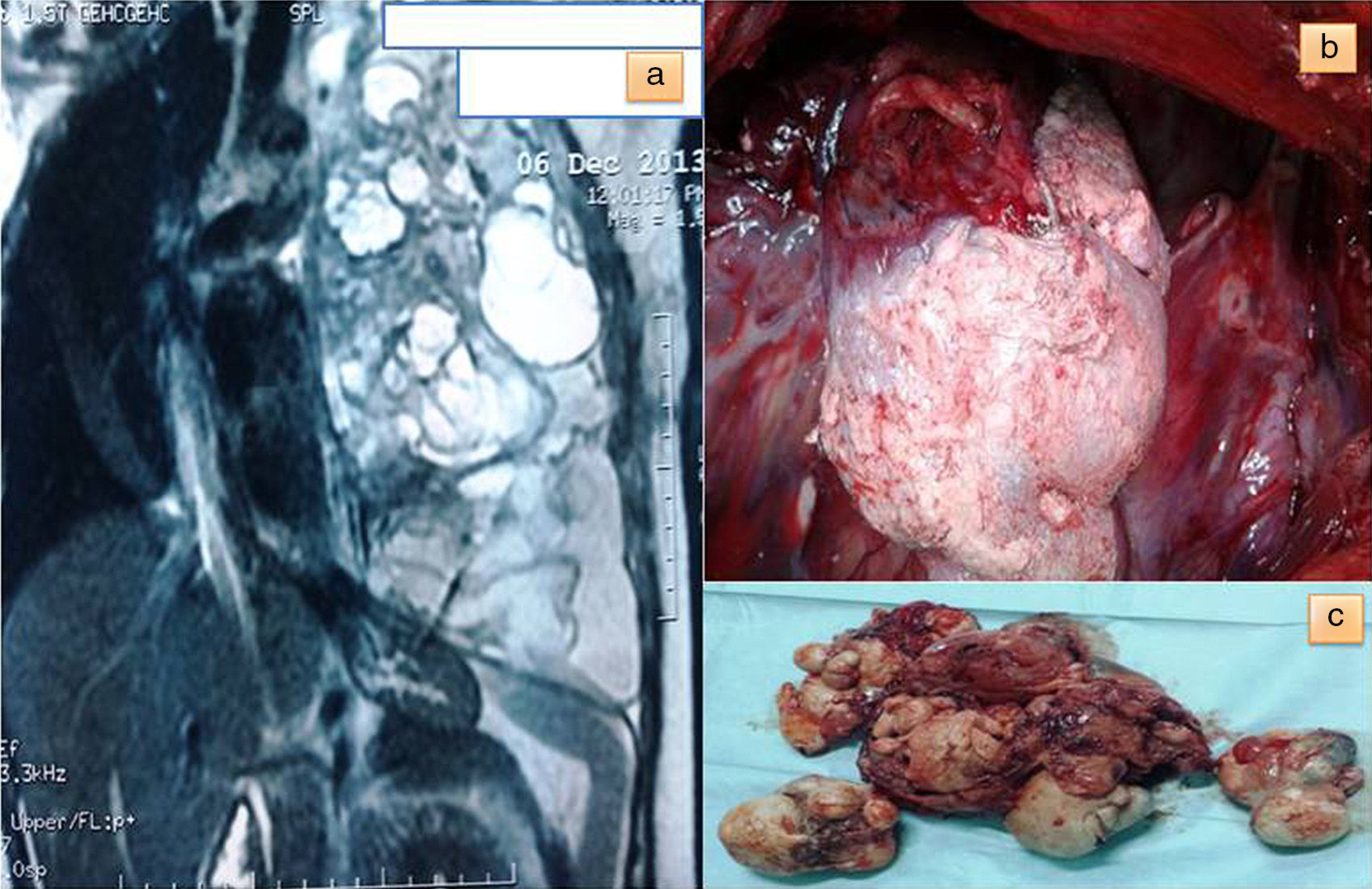
We report the case of a 21-year-old pregnant woman, admitted to the emergency department of our hospital with severe chronic dyspnea, minimal hemoptysis and premature labor. She was in week 28 of gestation, gravida 1, para 0. Gynecological examination revealed dilated external cervical orifice. SaO2 was 90% and blood pressure 90mmHg/60mmHg. Chest auscultation revealed absence of respiratory sounds in the left hemithorax, which was totally opaque on minimal exposure chest X-ray. Thoracocentesis was performed immediately, and a left chest tube was left in place to reduce dyspnea, producing 1500 cc of serous-sanguineous pleural fluid. Corticosteroid (betamethasone) was administered to accelerate fetal lung maturation. Three days later, after stopping premature labor, a Cesarean section was successfully performed with the birth of a healthy boy. Chest computed tomography (CT) and magnetic resonance imaging (MRI) (Fig. 1) revealed a mediastinal tumor occupying the whole left hemithorax, with massive right mediastinal shift. The tumor contained cystic spaces and discrete areas of soft tissue and fat, consistent with probable mature teratoma. Serum alpha-fetoprotein (AFP) and human chorionic gonadotropin (hCG) levels were normal. During posterolateral thoracotomy, the giant tumor was seen to have adhesions to the left lung, which was completely collapsed. The tumor contained organoid structures (hair), consistent with teratoma (Fig. 1b). Surprisingly, good lung re-expansion was achieved after full tumor resection (Fig. 1c). Histological diagnosis was mature teratoma. Positive estrogen and progesterone receptors were detected in resected tumor tissue.
Sixty percent of teratomas are located in the anterior mediastinum, and 88% are mature.1 Mature teratoma is often asymptomatic and protrudes from one hemithorax. On CT, it is seen as a mass containing fat, calcifications or cystic changes. The benign nature of these lesions is confirmed by lack of activity on FDG-PET.2 MRI is useful for obtaining an accurate map of surrounding anatomical structures for surgical resection of the tumor.
The only curative treatment available for teratoma is surgical intervention, usually performed via sternotomy or thoracotomy, to relieve symptoms of compression and prevent transformation to malignancy.
Correct diagnosis and treatment are based on total tumor resection, although complete resection is not essential, since the local recurrence rate is low.3 Adjuvant treatment is unnecessary, as prognosis for mature teratoma is good.4
In pregnant women, radiation applied to the chest is considered safe if the abdomen is protected,5 so chest X-ray is formally indicated to avoid misdiagnosis of unexplained dyspnea in a pregnant woman.
This large chest tumor causes decline in lung function, and pleural effusion may increase due to hormone changes and mechanical factors associated with pregnancy.
To conclude, the appearance of these tumors during pregnancy is likely to involve real diagnostic and therapeutic issues.
Conflict of InterestThe authors have no conflict of interests to declare.
Please cite this article as: El Hammoumi M, Benosman A, Kabiri EH. Teratoma gigante manifestado en el embarazo y causante de insuficiencia respiratoria. Arch Bronconeumol. 2015;51:250–251.







