



In Legionella infections, pleural affectation is not infrequent, but the formation of empyema and the isolation of the microorganism in the pleural liquid are considered exceptional.1
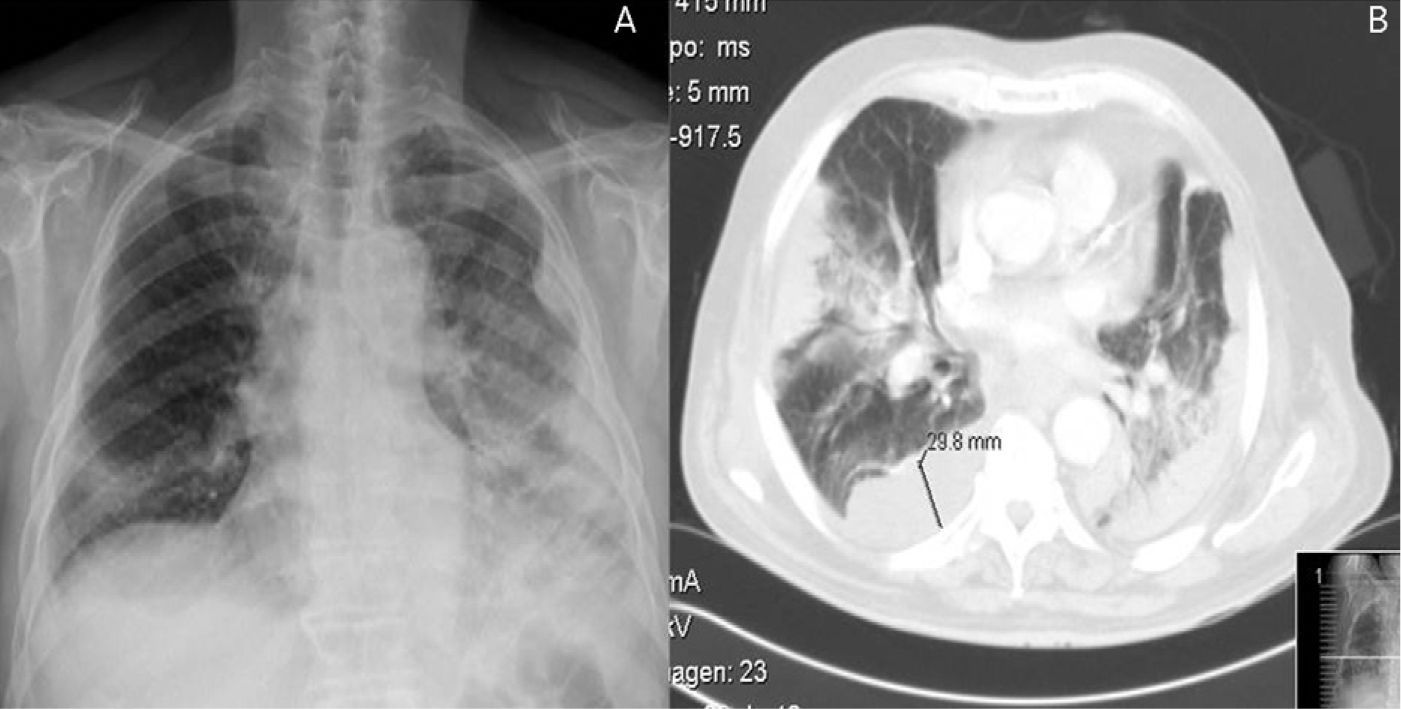
A 65-year-old male, ex-smoker of 40 pack-years with no other history of interest, was admitted due to dyspnea, cough with very little expectoration of mucus and pleuritic-type pain in the left hemithorax that had been evolving over the previous 5 days without fever. Upon physical examination, we observed tachypnea; pulmonary auscultation revealed diminished vesicular murmur and wet crackles in the lower third of both hemithoraces as well as pleural friction rub in the lower third of the left hemithorax. The blood analysis showed evidence of leukocytosis (21 800/mm3) with neutrophilia (95%); C reactive protein, 34mg/dl. Posteroanterior radiography revealed left pleural thickening, bilateral alveolar-interstitial pattern, condensation in both pulmonary bases and blunting of the left costophrenic angle (Fig. 1A). Thoracic computed tomography (CT) 48h later demonstrated extensive bilateral alveolar condensation with predominantly right pleural effusion, several left pleural collections and inflammatory lymphadenopathies (Fig. 1B). Given the presence of acute-phase reactants and the radiological findings, antibiotic treatment was begun with intravenous levofloxacin and beta-lactams, and after the CT bronchoscopy was performed, which was compatible with an acute suppurative process, and thoracocentesis, which showed a purulent exudate, with a pH of 7.22; 22 730 leukocytes/mm3; 73% neutrophils; 27% lymphocytes; glucose, 110mg/dl; LDH, 2371U/l, and proteins, 4.5g/dl. Right thoracic drainage was begun with the instillation of 100 000IU of urokinase and the emission of 500ml over the course of 3 days. Organized left pleural effusion was treated conservatively as there was limited pleural space. The Legionella antigens in urine were positive, and 7 days later L. pneumophila growth was observed in the pleural liquid on BCYEα medium and later confirmed by PCR-STB (sequence-based typing). The other tests (bronchial aspirate culture, protected telescoping catheter, blood cultures) were negative. The evolution of the patient was favorable, with progressive remission of the symptoms and of the pulmonary infiltrates.
Disease caused by Legionella usually runs its course with cough, fever, anorexia, myalgia, cephalalgia and pleuritic pain in one-third of patients, in addition to other non-pulmonary manifestations. A small amount of pleural effusion has been reported in 10%–50% of the patients, and this may precede the development of the parenchymatous process. Empyema due to L. pneumophila and the isolation of the germ in the pleural liquid are both uncommon in the literature.1,2 Few cases have been reported that run their course with pneumonia and empyema due to this microorganism, especially in immunosuppressed patients and transplant recipients.3,4 Winn and Myerowitz5 studied the necropsies of 74 patients diagnosed with legionellosis with pleural effusion and only in 5 cases was the volume more than 200ml, with findings for empyema in 2 cases. Legionella cultures in BCYEα have been the gold standard for the diagnosis of legionellosis, with a sensitivity from 20% to 95% and specificity near 100%.6 Rarely have positive cultures been obtained from the pleural liquid as in our case. We conclude that, although empyema due to L. pneumophila is infrequent, it should be taken into consideration and, therefore, in geographical regions with a high prevalence, Legionella should be included in the protocol of invasive respiratory sample studies.
Please cite this article as: Ferrufino E, et al. Empiema por Legionella pneumophila. Arch Bronconeumol. 2012; 48: 102-103.







