

Inhalation of carbon monoxide (CO) can result in poisoning, with symptoms ranging from mild and nonspecific to severe, or even death. CO poisoning is often underdiagnosed because exposure to low concentrations goes unnoticed, and threshold values for normal carboxyhemoglobin vary according to different authors. The aim of our study was to analyze carboxyhemoglobin (COHb) levels in an unselected population and detect sources of CO exposure.
MethodsIn a cross-sectional descriptive study, we analyzed consecutive arterial blood gas levels processed in our laboratory. We selected those with COHb≥2.5% in nonsmokers and ≥5% in smokers. In these cases a structured telephone interview was conducted.
ResultsElevated levels of COHb were found in 64 (20%) of the 306 initial determinations. Of these, data from 51 subjects aged 65±12 years, 31 (60%) of which were men, were obtained. Mean COHb was 4.0%. Forty patients (78%) were non-smokers with mean COHb of 3.2%, and 11 were smokers with COHb of 6.7%. In 45 patients (88.2%) we detected exposure to at least one source of ambient CO other than cigarette smoke.
ConclusionsA significant proportion of individuals from an unselected sample had elevated levels of COHb. The main sources of CO exposure were probably in the home, so this possibility should be explored. The population should be warned about the risks and encouraged to take preventive measures.
La inhalación de monóxido de carbono (CO) puede producir intoxicación, ocasionando desde una sintomatología inespecífica hasta la muerte. Muchas veces hay infradiagnóstico ya que exponerse a concentraciones bajas pasa inadvertida, y los valores umbral de normalidad para la carboxihemoglobina varían según distintos autores. El objetivo de nuestro trabajo fue analizar los niveles de carboxihemoglobina (COHb) en una población no seleccionada y detectar las fuentes de exposición al monóxido de carbono.
MétodosCon un diseño transversal y descriptivo, se analizaron consecutivamente las gasometrías arteriales procesadas en nuestro laboratorio. Se seleccionaron aquellos que tenían una COHb≥2,5% en no fumadores y≥5% en fumadores. A los casos seleccionados se realizó entrevista telefónica estructurada.
ResultadosDe 306 valoraciones iniciales, 64 casos (20%) tenían valores elevados de COHb y se obtuvieron datos de 51, 31 (60%) varones, de 65±12 años. La media de COHb fue de 4,0%. Cuarenta pacientes (78%) eran no fumadores con niveles de COHb de 3,2% y 11 fumadores con niveles de COHb de 6,7%. En 45 pacientes (88,2%) se detectó exposición a al menos una fuente de producción de CO ambiental distinta al humo del tabaco.
ConclusionesUn porcentaje relevante de individuos de una muestra no seleccionada tiene valores elevados de COHb. Posiblemente las principales fuentes de exposición estén en el domicilio particular, por lo que debe explorarse esta posibilidad, alertar sobre los riesgos y estimular la toma de medidas preventivas.
Carbon monoxide (CO) is an odorless, colorless, toxic gas produced by incomplete combustion of hydrocarbons. Its affinity for hemoglobin is 250 times greater than that of oxygen. The oxygen–hemoglobin bond is broken by CO, which then binds permanently to this molecule to form carboxyhemoglobin (COHb). Sixty percent (60%) of the CO in our environment is a product of burning tobacco, biomass and fossil fuel, and 40% occurs naturally.
Inhaling CO can be very harmful to health. It causes poisoning, with clinical manifestations ranging from non-specific symptoms to death.1 Prolonged exposure to even low levels of CO may have adverse effects, particularly on the cardiovascular and nervous systems.2 Underdiagnosis can be very common, since low but persistent concentrations of CO often go undetected, leading to COHb levels increasing until chronic poisoning (CP) occurs; in many cases, medical attention is not even sought (occult poisoning, OP).3 Furthermore, normal values for COHb vary according to different authors and the characteristics of the population under study.
It is generally agreed that in non-smokers, the percentage of COHb in blood should be lower than 2%, while in smokers it can reach up to 10%.3–7 High levels of COHb may frequently be attributed to tobacco use, but another common cause is inhalation of CO in the home or the workplace. These situations must be identified in order to implement protective measures and prevent CO poisoning.
The hypothesis of our study was that COHb analysis in a non-selected population may identify individuals with high COHb levels who could be exposed to sources of CO in the home or at work. The aim of our study was to analyze COHb levels in an unselected population and to detect possible sources of carbon monoxide exposure.
Materials ad MethodsStudy Design and Study GroupsThis is a cross-sectional, descriptive study in which arterial blood gases processed in our lung function laboratory on 9 randomly selected days in the month of April 2013 were analyzed consecutively. Samples were obtained and processed according to the SEPAR lung function evaluation procedure manual, using a Gem® Premier™ 4000 (Inc. Lexington, MA, USA) gasometer.8
Following a preliminary examination of all cases, non-smokers with COHb≥2.5% and smokers with COHb≥5% were selected, according to the criteria proposed in the literature.3,5,9,10 The individuals selected were invited to participate (verbal consent) in a telephone interview and were given information on how to maximize protective measures in their environment. The study was approved by the ethics committee of our hospital.
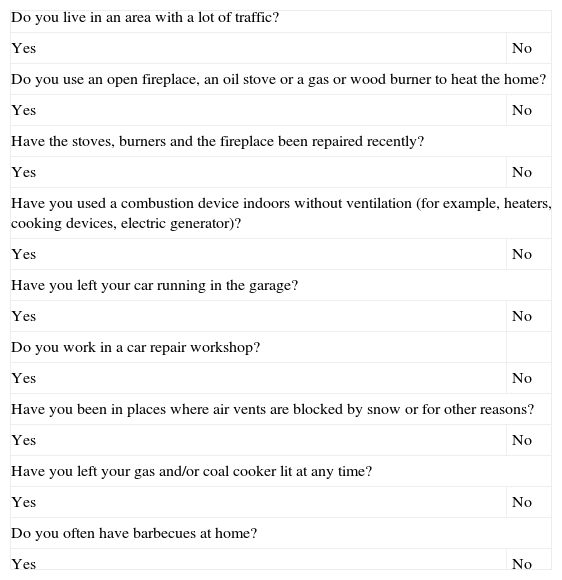
Data CollectionThis study was performed in the central region of Asturias (Healthcare Region IV) during the month of April 2013. All selected patients who agreed to participate underwent a telephone interview within 4–6 weeks after blood gases were determined. The interview collected data on age, sex, habitat (rural or urban), disease history, smoking habit, work outside the home, sources of exposure to CO in the home or at work11 (Annex 1) and related symptoms. This survey was based on the detailed environmental exposure questionnaire developed by the Society of General Practitioners of Ontario, Canada, adapted for CO exposure.
StatisticsIt was estimated that 298 blood gas determinations would be required for a 95% confidence level and a confidence interval of 6. Quantitative variables are expressed as mean and standard deviation and analyzed by comparison of means (Student t-test). Qualitative variables are expressed as percentages and were analyzed using the Chi-squared test. P<.05 was considered statistically significant.
ResultsThe initial sample of 306 arterial blood gases evaluated consisted of 67% males with a mean age of 69 (standard deviation [SD]: 12) years. The median level of COHb was 2.1% (0.3%–14%). A total of 79% were non-smokers or former smokers. Sixty-four (64) cases (20%) had COHb levels above the preset limit, of which 13 were excluded: 6 had died before the telephone interview could be conducted, 5 could not be located and 2 did not wish to participate. No differences in sex, age and mean COHb values were found between these 13 cases and the group of subjects who were included.
A total of 51 cases (Fig. 1) were studied, of which 31 (61%) were men, aged 65 (±12) years, 53% lived in a rural environment, and 56% were retired and stayed at home most of the day. Mean COHb level was 4.04% (SD 1.9). Forty (40) patients (78%) with IC were non-smokers with a COHb level of 3.2% (SD 1.1) and 11 were smokers with a COHb level of 6.7% (SD 1.7). Of the non-smokers, 7 (17%) reported passive exposure to tobacco smoke but their COHb levels were not significantly different from those of other non-smokers.

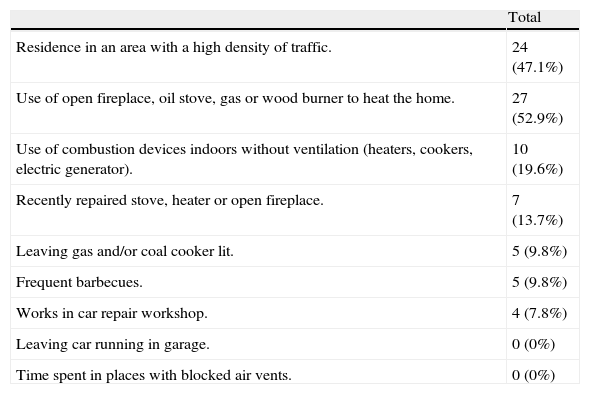
Exposure to sources of environmental CO other than tobacco smoke was detected in 45 cases (88.2%) (Table 1). Exposure to a single source was reported by 18 subjects, while 27 reported multiple sources of exposure. Symptoms were detected in 11 subjects (21%), the most common being morning headache. Only one of the subjects interviewed had a CO detector in the home.
Possible Sources of Carbon Monoxide Exposure in the Environment.
| Total | |
| Residence in an area with a high density of traffic. | 24 (47.1%) |
| Use of open fireplace, oil stove, gas or wood burner to heat the home. | 27 (52.9%) |
| Use of combustion devices indoors without ventilation (heaters, cookers, electric generator). | 10 (19.6%) |
| Recently repaired stove, heater or open fireplace. | 7 (13.7%) |
| Leaving gas and/or coal cooker lit. | 5 (9.8%) |
| Frequent barbecues. | 5 (9.8%) |
| Works in car repair workshop. | 4 (7.8%) |
| Leaving car running in garage. | 0 (0%) |
| Time spent in places with blocked air vents. | 0 (0%) |
In this study we found that an analysis of COHb values in unselected individuals detected 16% with raised values, of whom 88% were exposed to sources of CO other than tobacco smoke in the workplace or home environment, suggesting a population at risk of CO poisoning.
CO poisoning is the most common worldwide cause of injury and death due to poisoning.12 It is estimated that in Spain between 5000 and 10000 subjects suffer CO poisoning annually, with a mean of 125 deaths per year. Deaths most commonly occur in the winter months, due to the domestic use of ovens, gas stoves, wood burners and open fireplaces that are either poorly maintained or used in areas with little ventilation,13,14 explaining the importance of detecting at-risk situations and individuals. The greatest risk appears to be in the home15,16 and it is important to note that in our study 56% of the individuals spent most of the day at home, and the most commonly reported sources of exposure were emissions from “open fireplaces, oil-burning stoves, gas or wood burners for heating the home”.
Tobacco use is the major cause of elevated COHb2,5,9 levels and must be the primary suspect when these are detected. Accordingly, our study subjects were questioned specifically about this point, and 62 individuals (20%) were reported as active smokers. This figure is close to the 21.7% reported as habitual tobacco users in the Asturias health survey of 2011–2012.17 However, since smokers can also be exposed to other sources of CO, different cutoff values for COHb were used in smokers and non-smokers.
Our cutoff points were selected on the basis of published studies.6,7,10,18,19 In a population of 2104 non-smokers, Casan et al.6 found mean COHb levels in arterial blood gases of 1.65%. Puente-Maestu et al.7 reported mean arterial blood gas COHb of 1.53%, also in non-smokers. However, García Aroyo et al.18 reported a mean COHb level of 3.29% in non-smokers, probably due to the use of charcoal-burning stoves for heating the home, typical in rural areas. In a series of non-smokers with chronic respiratory failure receiving home oxygen therapy, González Ruíz et al.10 also found that those who used charcoal burners for heating the home had a mean COHb level of 4.63% compared to the 2.15% level detected in those using central heating. In studies performed in urban populations in the United States and the United Kingdom, levels lower than 2% were found in non-smokers, while COHb levels in smokers were over 5%.2,4,5,20
These data suggest that COHb values may be subject to geographical variations associated with lifestyle habits, particularly the use of biofuels for heating the home. In our series, we detected a mean COHb value of 2.8% in non-smokers and 6.4% in smokers.
We would draw attention to the analysis of COHb levels and highlight the possibility that an individual may be exposed to a risk of poisoning at home or at work. This will permit the introduction of recommendations to reduce environmental risk, bearing in mind that the most severe complication of CO poisoning is death.
Our study is limited by the possible under-declaration of smoking habit, and the fact that CO emissions in the home were not measured to confirm the origin of the exposure. Nevertheless, recommendations on environmental risk reduction were shared with at-risk individuals. Another limitation of this study is the lack of data on concomitant diseases and the clinical or functional status of the subjects. The greatest strength of the study is that it highlights an underdiagnosed situation that can have potentially fatal consequences.
To conclude, we found that 16% of an unselected study population had COHb values considered to be elevated but that could not be attributed, at least exclusively, to a smoking habit. The main sources of exposure may be in the home, therefore this possibility must be investigated and subjects alerted to the risks of CO poisoning. In this respect, we suggest that an education and prevention program should be designed to raise awareness among the general population. Systematic evaluation of combustion devices and measurement of CO levels in the workplace and at home may be necessary for certain individuals.
Conflict of InterestThe authors declare that they have no conflict of interests.
| Do you live in an area with a lot of traffic? | |
| Yes | No |
| Do you use an open fireplace, an oil stove or a gas or wood burner to heat the home? | |
| Yes | No |
| Have the stoves, burners and the fireplace been repaired recently? | |
| Yes | No |
| Have you used a combustion device indoors without ventilation (for example, heaters, cooking devices, electric generator)? | |
| Yes | No |
| Have you left your car running in the garage? | |
| Yes | No |
| Do you work in a car repair workshop? | |
| Yes | No |
| Have you been in places where air vents are blocked by snow or for other reasons? | |
| Yes | No |
| Have you left your gas and/or coal cooker lit at any time? | |
| Yes | No |
| Do you often have barbecues at home? | |
| Yes | No |
Please cite this article as: Buchelli Ramirez H, Fernández Alvarez R, Rubinos Cuadrado G, Martinez Gonzalez C, Rodriguez Jerez F, Casan Clara P. Niveles elevados de carboxihemoglobina: fuentes de exposición a monóxido de carbono. Arch Bronconeumol. 2014;50:465–468.







