
It is unusual for pulmonologists to be familiar with the European and US regulations governing the administration of oxygen during air travel and each airline's policy in this respect. This lack of knowledge is in large part due to the scarcity of articles addressing this matter in specialized journals and the noticeably limited information provided by airlines on their websites. In this article we examine the regulations, the policies of some airlines and practical aspects that must be taken into account, so that the questions of a patient who may need to use oxygen during a flight may be answered satisfactorily.
En el entorno neumológico no es habitual conocer las normativas europeas y de EE. UU. que regulan la administración de oxígeno durante los viajes en avión y la política a tal respecto que cada compañía aérea tiene. Este desconocimiento se debe en gran parte a la escasez de artículos que abordan este tema en las revistas especializadas y a la llamativamente limitada información que nos proporcionan las aerolíneas en sus páginas web. En este artículo hemos abordado estas normativas, la política que siguen algunas aerolíneas y determinados aspectos prácticos que deberíamos tener en cuenta, para que podamos responder de forma satisfactoria a las preguntas que, en un momento puntual, nos pueda plantear un paciente que necesite utilizar oxígeno durante los viajes en avión.
According to data from the IATA (International Air Transport Association), which includes 240 airlines responsible for 84% of world air traffic, 2980 million passengers traveled by air in 2012.1 Respiratory problems constitute the second most common emergency on commercial flights, after syncope or pre-syncope.2 For this reason, patients with certain respiratory conditions who intend to travel by air should plan their trip well in advance.
The aim of this review is to provide healthcare professionals who treat these types of patients with updated information on the regulations governing the use of various oxygen sources during flights, and the policies of some airlines with regard to the transport of patients who may require oxygen therapy on board.
Current Regulations in EuropeRegulation (EC) No. 1107/2006 concerning the rights of disabled persons and persons with reduced mobility when traveling by air, was adopted by the European Parliament and the Council on 5 July 2006. “This text is part of the policy […] to combat discrimination against persons with disabilities and, more generally, with either permanent or temporary mobility problems”. Its main objective was “to allow disabled persons and persons with reduced mobility (PRM) to have the same possibility to travel by air as other citizens”.3
In 2009, the European Commission conducted 2 studies on the implementation of the aforementioned Regulation. The first, published on 11-4-2011, stated in point 2.2.4.3:
“The transport and supply of medical oxygen is handled in very different ways depending on the air carrier, and this causes uncertainty and much dissatisfaction among the passengers concerned. As currently worded, the Regulation [No. 1107/2006] does not provide a solution to the problem […]. Passengers who have a vital need for oxygen are either denied access to air transport or left in a situation of uncertainty concerning the conditions and costs of their transport.4
Medical oxygen is considered medical equipment and is therefore carried free of charge in accordance with the Regulation, but it is also subject to the legislation on dangerous goods and for this reason some airlines refuse to carry it on board and instead impose the use of their own oxygen. They consider this a service, which they provide free of charge or subject to a charge that can sometimes be high”.
The fourth axis of this document addresses the issue of medical oxygen and states that “The Commission will encourage negotiations about a voluntary commitment among all parties concerning the use of medical oxygen on board. Failing this, it will consider adopting a general approach […] by laying down binding rules” in relation to 3 issues:
- a)
“Establishing certification schemes for the air transport of certain types of equipment that are allowed on board, on condition that the maintenance requirements are met.
- b)
Setting a maximum fixed fare applicable throughout Europe for the supply of oxygen on board.
- c)
Providing passengers with clear and detailed information on the conditions of supplying medical oxygen on board”.
At the time of writing, we do not know if these negotiations have commenced, but they are becoming absolutely essential given the limited, if not non-existent, information that airlines offer patients who require oxygen therapy on board.
On 11 July 2012, a working document from the Commission on the Interpretative Guidelines on the application of Regulation (EC) No. 1107/2006, the aim of which was to improve and facilitate the application of said Regulation, stated5:
“As medical oxygen is among the types of medical equipment specifically mentioned in Annex II to the Regulation, disabled persons may carry oxygen within the cabin free of charge, subject to the equipment meeting any dangerous goods requirements (which are based on ICAO rules) and to advance notice to the carrier. Air carriers may choose to provide oxygen directly to the passenger. However, there is no obligation on air carriers to do so. Where oxygen is provided directly, the air carrier may charge for its provision. Where charges are imposed for the provision of medical oxygen, carriers may wish to consider offering it at a discounted rate. Carriers have to publish the cost of this service as part of the rules and restrictions applicable. Air carriers can require advance notice of the need for oxygen when a disabled person wishes to use the air carrier's own supply throughout a flight”.
There are few specifications in this document, and the interests of the carriers generally take precedence over the rights of passengers.
Current Regulations in the USAThe United States Department of Transportation (DOT), in an act published on 13 May 2008, which entered into force on 13 May 2009, called “Nondiscrimination on the Basis of Disability in Air travel”, sets out in Part 382.133 that any airline that takes off or lands in the United States, regardless of whether it is a US or foreign carrier, must permit the use of Federal Aviation Administration (FAA)-approved portable oxygen concentrators (POC), described in the section on “Factors to take into account when traveling with a POC”.6
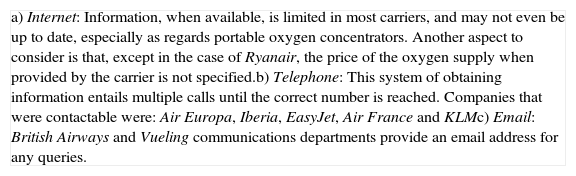
How to Find Airline InformationThe resources listed in Table 1 may be used to find information on the policies held by the various carriers.
Means for Obtaining Information on Airline Policies on Oxygen Therapy During Air Travel.
| a) Internet: Information, when available, is limited in most carriers, and may not even be up to date, especially as regards portable oxygen concentrators. Another aspect to consider is that, except in the case of Ryanair, the price of the oxygen supply when provided by the carrier is not specified.b) Telephone: This system of obtaining information entails multiple calls until the correct number is reached. Companies that were contactable were: Air Europa, Iberia, EasyJet, Air France and KLMc) Email: British Airways and Vueling communications departments provide an email address for any queries. |
The authors tried to obtain information by telephone or email from other airlines, but were unable to contact them or obtain further information.
To facilitate the information, the European Lung Foundation created a web page containing the policies pursued by the various carriers, which, in the case of some airlines, has not been updated since 2010.7 More recently, the European Federation of Allergy and Airway Diseases Patients Associations, in a booklet published in 2013, updated this information and, in particular, specified the importance of establishing a common policy, including the requirement that oxygen administration on aircraft should not be an economic burden for patients.8
Methods for Administering Oxygen to Patients who Require This Treatment During Air Travel- a)
Liquid oxygen. These devices are completely prohibited during flights by all airlines (as both cabin and hold luggage), as they are considered dangerous goods.
- b)
Oxygen cylinders. Most airlines do not permit patients to use their own cylinders on board. Of the European carriers that we have been able to contact: Iberia, Air Europa, Ryanair, Air France, KLM, British Airways, Vueling, and EasyJet, only the latter permits the use of oxygen cylinders on board, provided they do not exceed 50cm in length and 25cm in diameter. This airline also allows patients to carry a maximum of 2 cylinders at no extra cost. One important aspect is that the FAA prohibits all airlines from carrying oxygen cylinders for personal use on all flights to and from the United States.
- c)
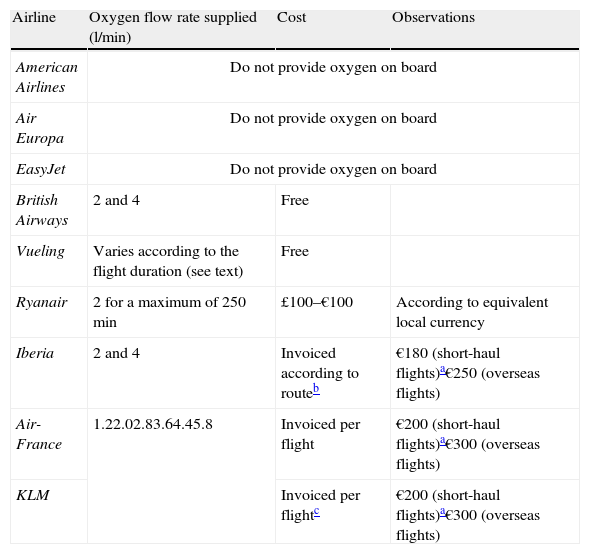
Oxygen supplied during the flight by the airline itself. Each airline applies its own policies in this regard: some supply oxygen at a cost (prices vary greatly), while others do not provide it at all (Table 2).
Table 2.Oxygen Flow Rate Supplied and Cost in Some Airlines.
Airline Oxygen flow rate supplied (l/min) Cost Observations American Airlines Do not provide oxygen on board Air Europa Do not provide oxygen on board EasyJet Do not provide oxygen on board British Airways 2 and 4 Free Vueling Varies according to the flight duration (see text) Free Ryanair 2 for a maximum of 250min £100–€100 According to equivalent local currency Iberia 2 and 4 Invoiced according to routeb €180 (short-haul flights)a€250 (overseas flights) Air-France 1.22.02.83.64.45.8 Invoiced per flight €200 (short-haul flights)a€300 (overseas flights) KLM Invoiced per flightc €200 (short-haul flights)a€300 (overseas flights)
When oxygen is supplied, it is generally at a (continuous) flow rate of 2–4l/min, as in the case of Iberia, Air Europa, and British Airways. Air France, KLM, and Lufthansa, meanwhile, use a new oxygen administration system called Wenoll WS 120, which delivers oxygen on demand with flow rates of 1.2, 2.0, 2.8, 3.6, 4.4 or 5.8l/min. On short-haul flights, Vueling can supply oxygen at 6l/min for flights under 1h and 30min, and up to 8l/min for flights under 1h and 12min. For long-haul flights, the maximum supply is 4l/min for flights longer than 3h and 30min, or 2l/min for flights up to a maximum of 6h and 30min. Ryanair only provide oxygen at a flow rate of 2l/min for a maximum of 250min, and do not accept passengers who require continuous oxygen supply for longer than the maximum time indicated. Depending on the carrier, the oxygen is administered using a mask (Iberia and British Airways) or nasal cannulae (Air France and KLM); nevertheless, at least in the case of Iberia, if the patient wishes to use nasal cannulae not supplied on board, they must bring their own.
Airlines that provide oxygen on board can place a limit on the maximum number of passengers who can be catered for on a particular flight (1 passenger in the case of British Airways and up to 3 on Air France and KLM); the maximum number on Iberia will depend on the oxygen availability of the carrier at any given time. This eventuality is resolved in all cases when the patient travels with their own POC.
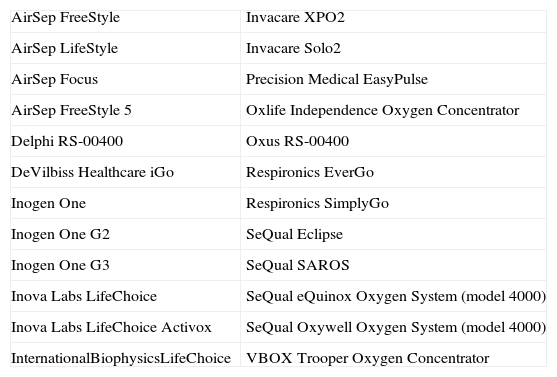
Factors to Take Into Account When Traveling With a Portable Oxygen ConcentratorAt present, the FAA has approved 24 POCs for use during flights (Table 3).9 Most carriers permit the use of these devices. There are various FAA-approved, therefore permitted, POC models, but not all are equally accepted by all airlines. Therefore, it is very important for the patient to be well informed, and to check that their particular POC is approved by their airline of choice. Iberia, Air Europa, EasyJet, British Airways, Air France, and KLM currently permit the 24 approved POCs to be used on their flights; Vueling does not place any restrictions on the type of POC, provided that it does not exceed the size permitted for hand baggage, so in practice, patients can fly with any POC currently on the market.
List of the 24 FAA-Approved Portable Oxygen Concentrators.
| AirSep FreeStyle | Invacare XPO2 |
| AirSep LifeStyle | Invacare Solo2 |
| AirSep Focus | Precision Medical EasyPulse |
| AirSep FreeStyle 5 | Oxlife Independence Oxygen Concentrator |
| Delphi RS-00400 | Oxus RS-00400 |
| DeVilbiss Healthcare iGo | Respironics EverGo |
| Inogen One | Respironics SimplyGo |
| Inogen One G2 | SeQual Eclipse |
| Inogen One G3 | SeQual SAROS |
| Inova Labs LifeChoice | SeQual eQuinox Oxygen System (model 4000) |
| Inova Labs LifeChoice Activox | SeQual Oxywell Oxygen System (model 4000) |
| InternationalBiophysicsLifeChoice | VBOX Trooper Oxygen Concentrator |
- 1.
Airlines cannot guarantee the availability of electrical connections and/or a power supply inside the aircraft. Therefore, the passenger must carry sufficient batteries to supply power to their medical equipment for the entire time it is in use.
- 2.
The number of batteries that the patient must carry for their POC should be calculated by their doctor, not by the airline, and must be sufficient to cover the entire duration of the flight, as well as extra time in case of delays. Although each company determines their own delay time, in general, most airlines state that the passenger should carry batteries to power the device for not less than 150% of the flight duration (Iberia, Air Europa, Air France, and KLM), i.e. if the trip lasts 6h, the patient should take sufficient batteries for the POC to work for 9 in-flight hours. However, in the case of EasyJet, the passenger must carry sufficient batteries to cover the duration of the flight plus 2 additional hours, while on Vueling, the customer is responsible for taking the spare batteries that they consider sufficient to cover their needs.
- 3.
Spare batteries must be packaged to protect them against short circuits or damage. According to the “Lithium Battery Guidance Document” published by the IATA and revised this year, one of the ways of preventing short circuits is to place each battery in one of the plastic bags generally used for transporting liquids or toiletries.10
- 4.
The FAA distinguishes 2 types of lithium batteries: non-rechargeable metal batteries and rechargeable batteries, known by the abbreviation Li+ (lithium ion). Lithium ion batteries which do not exceed 100W/h (used in cell phones) can be carried as cabin baggage with no restrictions on the number, provided that this is proportional to the number of devices that the patient is carrying and the duration of the trip. With respect to medium-power lithium ion batteries (>100 and ≤160W/h), which are the type used in POCs, the IATA explicitly states that only 2 spare batteries may be carried.9 As of 7 February 2014, Iberia, Air Europa, Ryanair, EasyJet, Air France, and KLM allow patients to fly with the POC and the number of batteries needed, even when this is more than 2. However, this results in the paradox that the airline allows the passenger to take the number of batteries needed, but airport security (AENA in Spain) prohibits more than 2 batteries to be taken through security, in accordance with IATA regulations. British Airways and Vueling do not permit more than 2 spare batteries to be carried on their flights.
- 5.
Carriers reserve the right to refuse carriage to those patients who do not have the correct FAA-approved equipment and sufficient batteries, or who have not followed the correct procedures required by the airlines.
- 6.
POCs and batteries can be carried as cabin baggage, and are not restricted by number of pieces or size, i.e. as they are not counted, a carry-on bag may be taken on board at no extra cost.
- 7.
The airline medical department may decide that some passengers with disability must travel accompanied by a caregiver/assistant, and in some cases, if the disability is severe, by a doctor or registered nurse, whose fees (including the price of the flight) must be met by the patient. In the case of patients who need to use oxygen on board, Iberia, Air Europa, EasyJet, Ryanair, Vueling, Air France, KLM, and British Airways allow these passengers to travel alone, provided that they know how to correctly manage the POC and can go to the bathroom unaided.
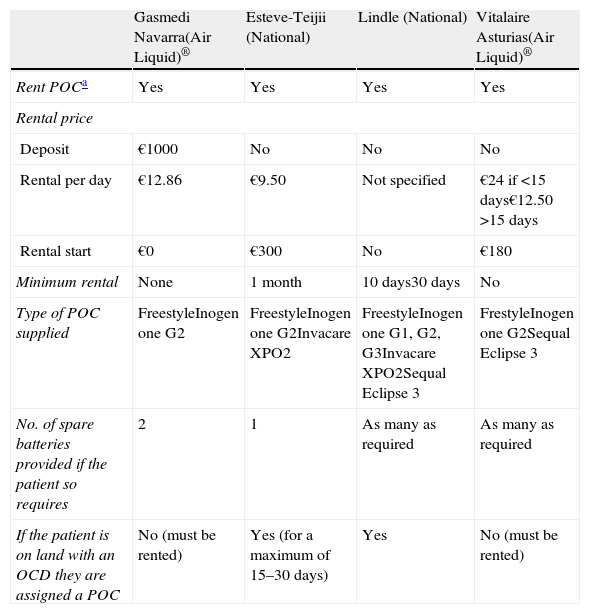
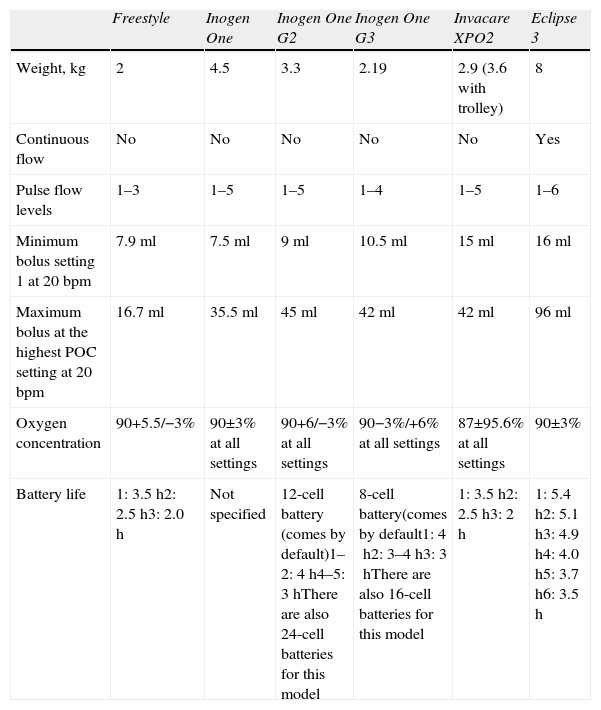
There are several Internet companies specializing in supplying oxygen for specific or short periods of time. In these cases, it may be more useful to ask the patient to contact one of their local home respiratory therapy (HRT) suppliers. Table 4 shows the policies of some Spanish HRT supply companies with respect to renting POCs, while Table 5 shows the characteristics and battery life of the POCs supplied by these companies.
Policies of Some Companies That Supply Home Respiratory Therapies With Respect to Renting Portable Oxygen Concentrators as of February 2014.
| Gasmedi Navarra(Air Liquid)® | Esteve-Teijii (National) | Lindle (National) | Vitalaire Asturias(Air Liquid)® | |
| Rent POCa | Yes | Yes | Yes | Yes |
| Rental price | ||||
| Deposit | €1000 | No | No | No |
| Rental per day | €12.86 | €9.50 | Not specified | €24 if <15 days€12.50 >15 days |
| Rental start | €0 | €300 | No | €180 |
| Minimum rental | None | 1 month | 10 days30 days | No |
| Type of POC supplied | FreestyleInogen one G2 | FreestyleInogen one G2Invacare XPO2 | FreestyleInogen one G1, G2, G3Invacare XPO2Sequal Eclipse 3 | FrestyleInogen one G2Sequal Eclipse 3 |
| No. of spare batteries provided if the patient so requires | 2 | 1 | As many as required | As many as required |
| If the patient is on land with an OCD they are assigned a POC | No (must be rented) | Yes (for a maximum of 15–30 days) | Yes | No (must be rented) |
Characteristics and Life of POC Batteries Supplied by HRT Companies.
| Freestyle | Inogen One | Inogen One G2 | Inogen One G3 | Invacare XPO2 | Eclipse 3 | |
| Weight, kg | 2 | 4.5 | 3.3 | 2.19 | 2.9 (3.6 with trolley) | 8 |
| Continuous flow | No | No | No | No | No | Yes |
| Pulse flow levels | 1–3 | 1–5 | 1–5 | 1–4 | 1–5 | 1–6 |
| Minimum bolus setting 1 at 20bpm | 7.9ml | 7.5ml | 9ml | 10.5ml | 15ml | 16ml |
| Maximum bolus at the highest POC setting at 20bpm | 16.7ml | 35.5ml | 45ml | 42ml | 42ml | 96ml |
| Oxygen concentration | 90+5.5/−3% | 90±3% at all settings | 90+6/−3% at all settings | 90−3%/+6% at all settings | 87±95.6% at all settings | 90±3% |
| Battery life | 1: 3.5h2: 2.5h3: 2.0h | Not specified | 12-cell battery (comes by default)1–2: 4h4–5: 3hThere are also 24-cell batteries for this model | 8-cell battery(comes by default1: 4h2: 3–4h3: 3hThere are also 16-cell batteries for this model | 1: 3.5h2: 2.5h3: 2h | 1: 5.4h2: 5.1h3: 4.9h4: 4.0h5: 3.7h6: 3.5h |
- 1.
Although each airline has its own policy, if a patient is on oxygen therapy on land, a hypoxia altitude simulation test (HAST) is, in principle, not necessary to determine the oxygen flow rate required during the flight. Iberia, Air Europa, EasyJet, British Airways, Air France, and KLM recommend that the patient's doctor calculate the oxygen flow rate required by the patient, without requesting that a HAST be performed.
- 2.
If the patient does not require oxygen on land, a flow rate of 2l/min is usually sufficient to correct hypoxemia during the flight; this can be doubled if required.11,12
- 3.
The oxygen flow rate needed to correct in-flight hypoxemia will not be the same in the patient's own POC as that supplied by the airline's system; it will depend on the type of device used, among other factors. In one study that evaluated 16 patients with chronic obstructive pulmonary disease (COPD) with a mean FEV-1 of 1.1 (37%±11% of predicted value), oxygen administration with a Free-Style portable concentrator at setting 2 increased the pO2 by 12mmHg, an increase similar to that obtained when oxygen is administered at 1l/min continuously or using an oxygen conserving device.13
- 4.
Not all POCs are the same. Fisher et al. evaluated the performance and improvement in blood gases obtained with 5 FAA-approved POCs (Freestyle, XPO2, Inogen One, EverGo, and Eclipse 3) with respect to the administration of oxygen at the equivalent of 2.8l/min using the WS 120 system, which is a compressed oxygen cylinder with a conserving device used by some airlines. At 2650m, the 2 lighter POCs, the Freestyle and the XPO2, had to be used at their maximum level (3/3 and 4/5, respectively) in order to increase pO2 by around 15mmHg, which significantly reduces the life of the battery, while the other 3 heavier POCs were able to improve PO2 by around 25mmHg, running at 50%–70% of their maximum level, similar to that obtained with the WS 120 system.14 Therefore, the choice of the best type of POC for each patient will depend on the degree of functional impairment and flight duration. If the patient has little functional impairment, the most lightweight POCs should be chosen, provided that the duration of the flight is short, while in more severe patients, heavier POCs should be used to ensure that the patient reaches a minimum pO2 of 50mmHg during the flight, as required in some guidelines.11,15
The patient's doctor must fill out a Medical Information/Incapacitated Passengers Handling Advice (MEDIF/INCAD) form in English or in the airline's official language. This document, based on IATA recommendations, consists of 2 parts: the INCAD, which can be filled out by the passenger or the travel agency in the case of passengers with special needs, e.g. passengers who are wheelchair-bound, blind, deaf or who have an illness that limits their understanding. Passengers suffering from a disease, who need to travel with oxygen or on a stretcher, must fill out the second part of the document, the MEDIF, in addition to the INCAD. In the MEDIF, the doctor must specify whether the patient is traveling with a POC, the make, model, number of batteries required, and the oxygen flow rate or pulses necessary to correct the hypoxemia. Once completed, the patient or travel agent must send it by fax or email to the airline at least 48–72h before the scheduled departure time. The airline will notify the patient, via email or SMS, at least 24h before take-off, whether their medical department has decided to deny or permit the passenger to fly, in which case it will inform the ground staff and cabin crew. When boarding, the patient must present a document issued by the company supplying the HRT, certifying that the POC is FAA-approved.
Medical Responsibility During FlightsOne aspect of air travel that healthcare professionals are unaware of concerns the extent of their responsibility in the event of an in-flight emergency. During flights, the aircraft is subject to the law in force in the airline's home country, regardless of the country over which it is flying. Thus, in Spain, France, and Germany, the code of professional ethics requires physicians to treat patients, while this obligation does not exist in the United Kingdom, Canada or the United States.16 In the latter, the Aviation Medical Assistance Act, popularly known as the Good Samaritan law (in effect since 1998) states that doctors who voluntarily treat an emergency cannot be tried except in the case of gross negligence.17
ConclusionsIn a globalized world in which air travel is increasingly more common, the lack of a common policy pursued by airlines with respect to the use of oxygen therapy during flights is, at the very least, striking. This heterogeneity is reflected in various aspects: administration of oxygen therapy on board by the carrier, costs stemming from this service, and even the ability to use FAA-approved concentrators.
The establishment of common, uniform criteria applicable to all airlines by the competent authorities would be an extremely positive step, making it easier for patients who use oxygen therapy to complete the numerous administrative formalities required for air travel.
FundingThe authors of this paper declare that they have not received any funding for conducting this study.
Conflict of InterestThe authors declare that they have no conflict of interests.
The authors of this paper would like to thank the following for their collaboration: Juan Piza and Álvaro Hebrero, Air Europa; Soledad, Iberia Medical Department; Almudena López Amor and Amparo Sierra, Air France and KLM; Elena Fernández Torres, Vueling; British Airways Medical Department; Solend, EasyJet; Victor Carabias, Gasmedi; Esther Ruiz, Esteve-Teijin; Ana Jordan, Lindle and Vitalaire, Asturias.
Please cite this article as: Cascante-Rodrigo JA, Iridoy-Zulet AA, Alfonso-Imízcoz M. Marco legal vigente y aspectos prácticos de la oxigenoterapia durante los viajes en avión. Arch Bronconeumol. 2015;51:38–43.







