


An 82-year-old female patient, lifelong resident of the United States who had not seen a doctor in over 50 years, was brought to the Emergency Department for failure to thrive. The patient had suffered from long-standing dysphagia. On arrival, she was tachycardic, tachypneic, and hypoxemic. There was a palpable neck mass with tracheal deviation. Arterial pH was 7.10 and PaCO2 was >126mmHg. She was intubated. Chest radiograph revealed marked widening of the mediastinum (Fig. 1A). Chest computed tomography (CT) demonstrated an anterior mediastinal mass exerting profound mass effect on surrounding structures (Fig. 1B–D). Clinical suspicion favored a giant goiter with substernal extension. CT-guided biopsy confirmed benign thyroid tissue. Echocardiography showed severely reduced right ventricular function. The patient developed rapidly progressive shock with multi-organ failure, which proved fatal. Autopsy was performed, revealing a 16cm×15cm×13cm multinodular goiter that weighed 1100g (normal 10–20g). The goiter nearly completely compressed the esophagus as well as the trachea and right-sided great vessels. The cause of death was deemed to be obstructive shock. Substernal goiter refers to growth of the thyroid gland from the neck caudally through the thoracic inlet and into the anterior mediastinal compartment. It is a rare occurrence, particularly in non-goitrogenic areas such as the United States or Europe, and even more rarely does it become sufficiently advanced to cause demise. The substernal goiter in this case is one of the largest, if not the largest, ever recorded: the major case series of resected substernal goiters report maximum specimen weights of under 1kg.1,2
 Portable chest radiograph showing mass-like widening of the mediastinum (asterisk). The path of the endotracheal tube demonstrates the rightward deviation of the trachea (arrow). (B) Axial section from chest computed tomography (CT) performed after administration of intravenous contrast and set to soft tissue window showing a giant, heterogeneous anterior mediastinal mass displacing the aortic arch (AA) laterally and the innominate vein (asterisk) anteriorly while compressing the trachea (thick arrow) and esophagus (thin arrow), both of which are markedly displaced from their normal locations. (C) Coronal reconstruction from the CT depicted in panel B highlighting the mass effect on the heart (asterisk), which is displaced inferolaterally, and on the pulmonary artery (PA), which is forced into a near-horizontal orientation by the mass. AA denotes the aortic arch cut in cross-section. (D) Saggital reconstruction from the same CT highlights the dramatically abnormal path of the superior vena cava (SVC), which wraps around the underside of the mass in a near-horizontal orientation.")
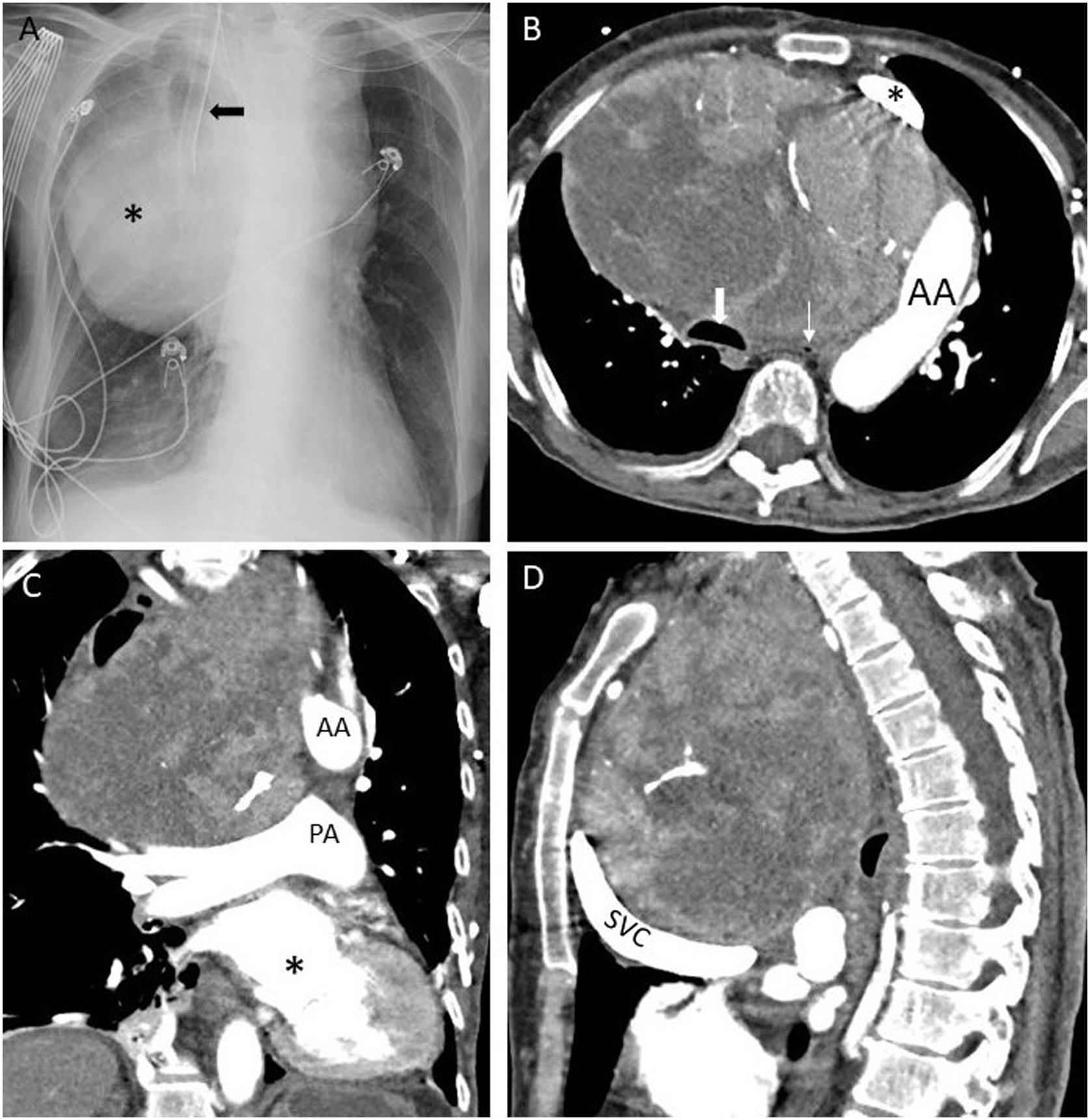
(A) Portable chest radiograph showing mass-like widening of the mediastinum (asterisk). The path of the endotracheal tube demonstrates the rightward deviation of the trachea (arrow). (B) Axial section from chest computed tomography (CT) performed after administration of intravenous contrast and set to soft tissue window showing a giant, heterogeneous anterior mediastinal mass displacing the aortic arch (AA) laterally and the innominate vein (asterisk) anteriorly while compressing the trachea (thick arrow) and esophagus (thin arrow), both of which are markedly displaced from their normal locations. (C) Coronal reconstruction from the CT depicted in panel B highlighting the mass effect on the heart (asterisk), which is displaced inferolaterally, and on the pulmonary artery (PA), which is forced into a near-horizontal orientation by the mass. AA denotes the aortic arch cut in cross-section. (D) Saggital reconstruction from the same CT highlights the dramatically abnormal path of the superior vena cava (SVC), which wraps around the underside of the mass in a near-horizontal orientation.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of InterestThe authors declare not to have any conflicts of interest.







