


A 72-year-old man with a history of idiopathic pleuroparenchymal fibroelastosis (PPFE) was admitted to our hospital due to sudden-onset dyspnoea, diagnosed as an exacerbation of PPFE (patient's serum KL-6 level: 2778U/mL and serum SP-D level: 1220ng/mL; Fig. 1A). Physical examination revealed an oxygen saturation of 86% while breathing ambient air and had diminished breath sounds. Corticosteroids and pirfenidone were administered despite no established evidence owing to limited available treatments.1 Although PPFE exacerbation improved (serum KL-6: 738U/mL and serum SP-D: 141ng/mL), the patient subsequently developed intractable pneumothorax (Fig. 1B). Despite the repeated use of blood-patch pleurodesis following chest drain insertion, air leaks persisted for 4 weeks. Given the infeasibility of a surgical intervention, endobronchial Watanabe spigots (EWS) were utilized to occlude the left B1+2a, b, and B10b (Fig. 1C and D). The air leaks ceased, and the chest tube was removed (Fig. 1E). This is a first report of improvement in intractable pneumothorax using EWS in a patient with PPFE. The EWS is a silicone bronchial blocker, which is an optional management strategy for patients with intractable pneumothorax and interstitial pneumonia when surgical treatment is not feasible.2,3
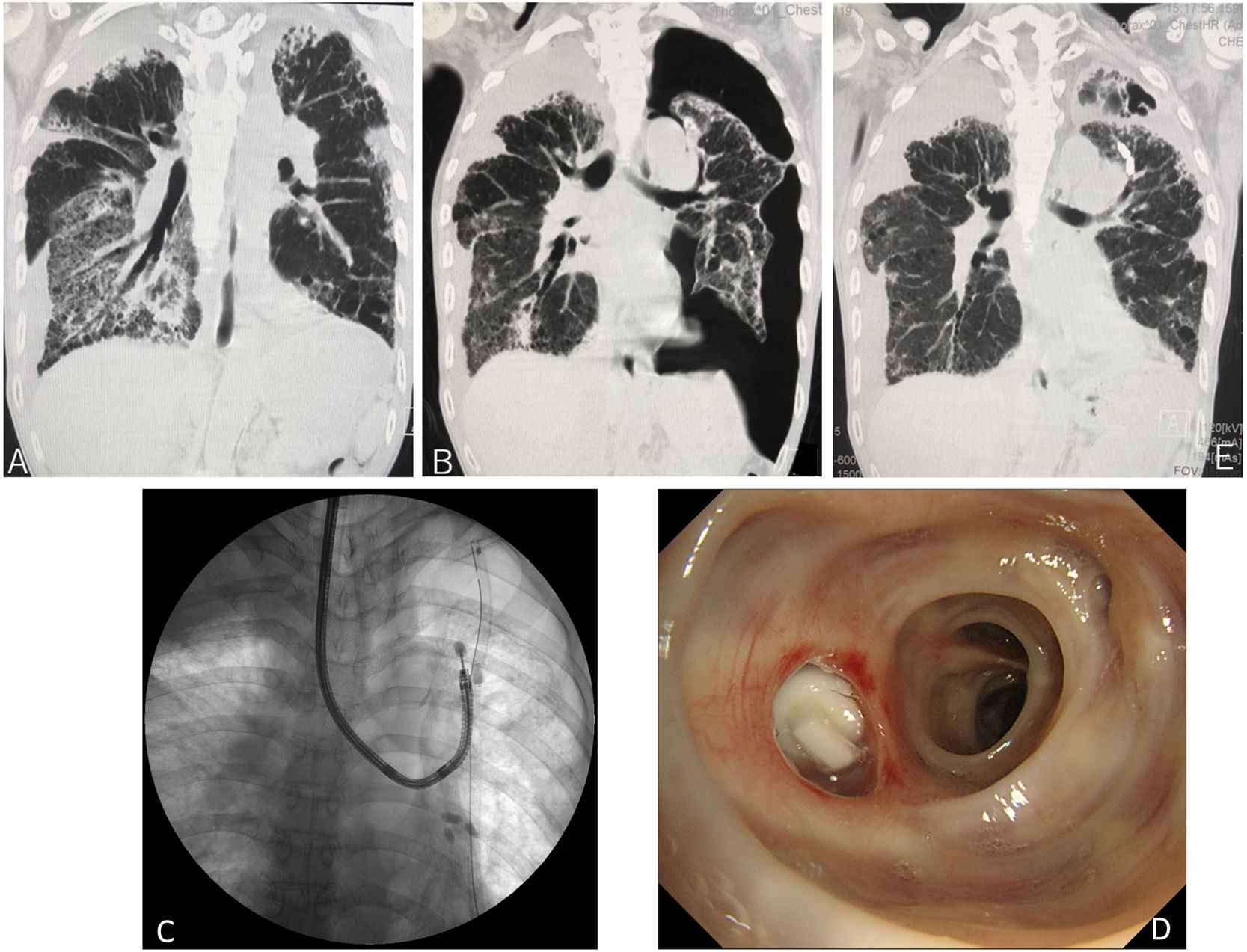
 Coronal reconstruction of chest computed tomography (CT) reveals traction bronchiectasis accompanied by a linear reticular shadow predominantly in the subpleural upper lobes, with surrounding pleural effusion. Additionally, ground-glass opacities (GGO) and a reversed halo-like shadow are predominantly observed in the right lower lobe, indicative of pleuroparenchymal fibroelastosis exacerbation. (B) After the administration of corticosteroids and pirfenidone, coronal reconstruction of chest CT reveals improvement of GGO and a reversed halo-like shadow. However, severe pneumothorax is observed in the left lung. (C) Fluoroscopic radiograph showing a left pneumothorax with a chest tube inserted into the left thoracic cavity. Additionally, endobronchial Watanabe spigots (EWS) are implanted at left B1+2 using a flexible bronchoscope. (D) The bronchoscopic findings reveal redness of the bronchial mucosa caused by the insertion of an EWS in the left B1+2b. (E) Coronal reconstruction of chest CT after EWS insertion demonstrates improvement of the inserted EWS, left pneumothorax, and right dominant GGO and reversed halo-like shadow. Abbreviations: CT, computed tomography; GGO, ground-glass opacities; EWS, endobronchial Watanabe spigot; PPFE, pleuroparenchymal fibroelastosis.")
(A) Coronal reconstruction of chest computed tomography (CT) reveals traction bronchiectasis accompanied by a linear reticular shadow predominantly in the subpleural upper lobes, with surrounding pleural effusion. Additionally, ground-glass opacities (GGO) and a reversed halo-like shadow are predominantly observed in the right lower lobe, indicative of pleuroparenchymal fibroelastosis exacerbation. (B) After the administration of corticosteroids and pirfenidone, coronal reconstruction of chest CT reveals improvement of GGO and a reversed halo-like shadow. However, severe pneumothorax is observed in the left lung. (C) Fluoroscopic radiograph showing a left pneumothorax with a chest tube inserted into the left thoracic cavity. Additionally, endobronchial Watanabe spigots (EWS) are implanted at left B1+2 using a flexible bronchoscope. (D) The bronchoscopic findings reveal redness of the bronchial mucosa caused by the insertion of an EWS in the left B1+2b. (E) Coronal reconstruction of chest CT after EWS insertion demonstrates improvement of the inserted EWS, left pneumothorax, and right dominant GGO and reversed halo-like shadow. Abbreviations: CT, computed tomography; GGO, ground-glass opacities; EWS, endobronchial Watanabe spigot; PPFE, pleuroparenchymal fibroelastosis.
The article does not contain the participation of any animal. Written informed consent was obtained from the patient for the publication of this report and accompanying images.
Patient ConsentObtained.
Authors’ ContributionsF.K. interpreted the data, drafted the original manuscript, and performed bronchoscopy. The author has reviewed and approved the final version of the manuscript.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of InterestThe author shall declare to have any conflicts of interest that may be affected directly or indirectly affect the content of manuscript.
The author thanks the patient for allowing the publication of this case report.







