


Exposure to secondhand smoke (SHS) is a public health problem worldwide.1 A recent study published in Archivos de Bronconeumología2 concluded that exposure to SHS caused 747 deaths in the Spanish population aged 35 and over in 2020 (279 deaths due to lung cancer and 468 due to ischemic heart disease). Of these deaths, six out of ten occurred in nonsmokers. In addition, if chronic obstructive pulmonary disease and cardiovascular disease were also considered in the analysis, the deaths attributed to SHS exposure would increase threefold.2 Health authorities should strive to eliminate exposure to SHS in the Spanish population in all age groups and in all settings. The burden of morbidity and mortality related to SHS exposure is avoidable.
In order to eliminate exposure to SHS, it is essential to have reliable and in-depth knowledge of the prevalence of exposure and to characterize those who are exposed. It is also crucial that health plans include SHS among the actions to be addressed and managed.
Regarding prevalence of exposure, the standardized collection of data through national and regional surveys in all Autonomous Communities (AC) of Spain is crucial. This permits the characterization of SHS at the population level, the accurate assessment of possible geographical and temporal variations, and facilitates the improvement of social awareness of this important risk factor. The European Health Survey in Spain and the Spanish Health Survey provide prevalence data on indoor exposure to SHS without differentiating by setting.3,4 These surveys are conducted in the Spanish population aged 15 years and older. Specifically focusing on the age group of 14–18 years, the National Survey on Drug Use in Secondary Education (ESTUDES) has been providing estimates of prevalence of exposure at home since its inception in 1996, with the latest version in 2023.5 However, for the adult population (15–64 years), the Spanish Survey on Alcohol and Other Drugs (EDADES) has not included questions assessing exposure to SHS since 2015.6 At the regional level, some AC in Spain carry out surveys that address exposure to SHS. However, the heterogeneity and variability in the questions included to ascertain exposure, as well as the different exposure settings considered, do not allow comparisons.7
To identify available actions oriented to control SHS exposure across all AC in Spain, we focused on two primary sources: AC health plans and addiction plans. The AC health plans play an important role as strategic tools for regional health planning and coordination; they delineate health policies and services and serve as a framework for all health initiatives within the AC. Meanwhile, the AC addiction plans are the primary tool for addressing substance use disorders and behavioral addictions by coordinating resources, goals, and interventions specific to these issues.
Although all 17 AC health plans cover tobacco use, only three assess SHS (Table 1). The health plan of Cantabria is the only one that incorporates prevalence data on exposure to SHS at home, work, and on public transport and private premises. This plan emphasizes the high mortality related to exposure to SHS and the broadly need to disseminate information on the adverse effects derived from such exposure; it also highlights the importance of tailoring this information to diverse segments of the population. The health plan of the Basque Country focuses on the evaluation of the decrease in SHS exposure in the first decade of the 21st century, while the health plan of the Principality of Asturias highlights the social inequalities in SHS exposure in children (Table 1).
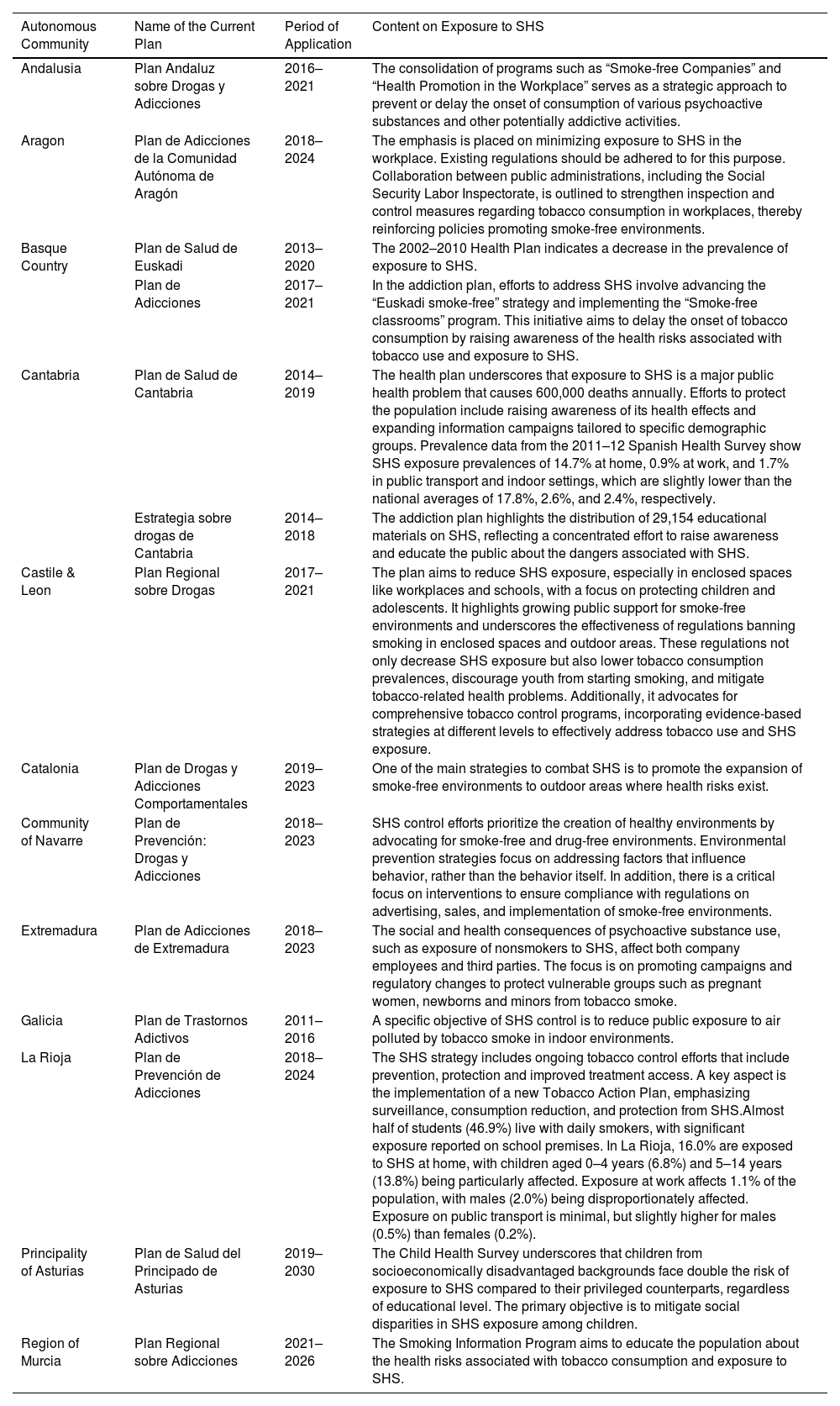
General Characteristics of the Autonomous Health Plans and of the Autonomous Addiction Plans With Specific Information on Exposure to Secondhand Smoke (SHS).
| Autonomous Community | Name of the Current Plan | Period of Application | Content on Exposure to SHS |
|---|---|---|---|
| Andalusia | Plan Andaluz sobre Drogas y Adicciones | 2016–2021 | The consolidation of programs such as “Smoke-free Companies” and “Health Promotion in the Workplace” serves as a strategic approach to prevent or delay the onset of consumption of various psychoactive substances and other potentially addictive activities. |
| Aragon | Plan de Adicciones de la Comunidad Autónoma de Aragón | 2018–2024 | The emphasis is placed on minimizing exposure to SHS in the workplace. Existing regulations should be adhered to for this purpose. Collaboration between public administrations, including the Social Security Labor Inspectorate, is outlined to strengthen inspection and control measures regarding tobacco consumption in workplaces, thereby reinforcing policies promoting smoke-free environments. |
| Basque Country | Plan de Salud de Euskadi | 2013–2020 | The 2002–2010 Health Plan indicates a decrease in the prevalence of exposure to SHS. |
| Plan de Adicciones | 2017–2021 | In the addiction plan, efforts to address SHS involve advancing the “Euskadi smoke-free” strategy and implementing the “Smoke-free classrooms” program. This initiative aims to delay the onset of tobacco consumption by raising awareness of the health risks associated with tobacco use and exposure to SHS. | |
| Cantabria | Plan de Salud de Cantabria | 2014–2019 | The health plan underscores that exposure to SHS is a major public health problem that causes 600,000 deaths annually. Efforts to protect the population include raising awareness of its health effects and expanding information campaigns tailored to specific demographic groups. Prevalence data from the 2011–12 Spanish Health Survey show SHS exposure prevalences of 14.7% at home, 0.9% at work, and 1.7% in public transport and indoor settings, which are slightly lower than the national averages of 17.8%, 2.6%, and 2.4%, respectively. |
| Estrategia sobre drogas de Cantabria | 2014–2018 | The addiction plan highlights the distribution of 29,154 educational materials on SHS, reflecting a concentrated effort to raise awareness and educate the public about the dangers associated with SHS. | |
| Castile & Leon | Plan Regional sobre Drogas | 2017–2021 | The plan aims to reduce SHS exposure, especially in enclosed spaces like workplaces and schools, with a focus on protecting children and adolescents. It highlights growing public support for smoke-free environments and underscores the effectiveness of regulations banning smoking in enclosed spaces and outdoor areas. These regulations not only decrease SHS exposure but also lower tobacco consumption prevalences, discourage youth from starting smoking, and mitigate tobacco-related health problems. Additionally, it advocates for comprehensive tobacco control programs, incorporating evidence-based strategies at different levels to effectively address tobacco use and SHS exposure. |
| Catalonia | Plan de Drogas y Adicciones Comportamentales | 2019–2023 | One of the main strategies to combat SHS is to promote the expansion of smoke-free environments to outdoor areas where health risks exist. |
| Community of Navarre | Plan de Prevención: Drogas y Adicciones | 2018–2023 | SHS control efforts prioritize the creation of healthy environments by advocating for smoke-free and drug-free environments. Environmental prevention strategies focus on addressing factors that influence behavior, rather than the behavior itself. In addition, there is a critical focus on interventions to ensure compliance with regulations on advertising, sales, and implementation of smoke-free environments. |
| Extremadura | Plan de Adicciones de Extremadura | 2018–2023 | The social and health consequences of psychoactive substance use, such as exposure of nonsmokers to SHS, affect both company employees and third parties. The focus is on promoting campaigns and regulatory changes to protect vulnerable groups such as pregnant women, newborns and minors from tobacco smoke. |
| Galicia | Plan de Trastornos Adictivos | 2011–2016 | A specific objective of SHS control is to reduce public exposure to air polluted by tobacco smoke in indoor environments. |
| La Rioja | Plan de Prevención de Adicciones | 2018–2024 | The SHS strategy includes ongoing tobacco control efforts that include prevention, protection and improved treatment access. A key aspect is the implementation of a new Tobacco Action Plan, emphasizing surveillance, consumption reduction, and protection from SHS.Almost half of students (46.9%) live with daily smokers, with significant exposure reported on school premises. In La Rioja, 16.0% are exposed to SHS at home, with children aged 0–4 years (6.8%) and 5–14 years (13.8%) being particularly affected. Exposure at work affects 1.1% of the population, with males (2.0%) being disproportionately affected. Exposure on public transport is minimal, but slightly higher for males (0.5%) than females (0.2%). |
| Principality of Asturias | Plan de Salud del Principado de Asturias | 2019–2030 | The Child Health Survey underscores that children from socioeconomically disadvantaged backgrounds face double the risk of exposure to SHS compared to their privileged counterparts, regardless of educational level. The primary objective is to mitigate social disparities in SHS exposure among children. |
| Region of Murcia | Plan Regional sobre Adicciones | 2021–2026 | The Smoking Information Program aims to educate the population about the health risks associated with tobacco consumption and exposure to SHS. |
On the other hand, all the AC in Spain have specific addiction plans focusing on psychoactive substance consumption. The addiction plans of Castile-La Mancha, the Community of Madrid, the Balearic Islands, the Canary Islands, and the Principality of Asturias cover tobacco use but not exposure to SHS. Notably, La Rioja includes data on prevalence of exposure to SHS in its addiction plan. Specifically, it includes prevalence of exposure at home, work, on educational premises, and public and private transport in both pediatric and adult populations. The addiction plans of Andalusia, Aragon, Cantabria, Castile & Leon, Catalonia, Extremadura, La Rioja, the Community of Navarre, the Basque Country, and the Region of Murcia, include objectives, strategic actions or interventions aimed to: (1) Raise public awareness of the health risk related to SHS exposure; (2) Protect the general population against SHS exposure, particularly among vulnerable groups such as pregnant women and minors; (3) Reinforce smoke-free policies, especially in the family, workplace, and school settings; and (4) Decrease the initiation of tobacco consumption among young people, as well as the burden of disease and mortality attributed to tobacco (Table 1). In summary, while each AC has adopted its own strategies to address SHS in their addiction plans, there is a shared commitment to promoting smoke-free environments and educating the population about the health risks associated with tobacco use and exposure to SHS.
It is noteworthy that Cantabria and the Basque Country are the only AC that contain actions oriented to control exposure to SHS in both their health and addiction plans. Actions or strategies aimed at reducing the prevalence of exposure to SHS are more frequent in addiction plans than in health plans. Regional health plans do not identify SHS as a health problem. This is evidenced by the fact that only three of them assess SHS exposure.
The AC are free to include measures aimed at controlling exposure to SHS in other strategic documents such as tobacco control plans, as in the case of the Community of Valencia, or respiratory health plans, in Galicia. However, it would be beneficial to include this information in more encompassing planning documents, such as health plans.
Spain enacted firstly a partial comprehensive smoke-free legislation in 20068 and 2011,9 which were associated with an immediate decrease in both respiratory diseases10 and prevalence of exposure to SHS among nonsmokers,11 and a slight decrease in prevalence among smokers.12,13 The recently presented national smoking control plan (“Plan Integral de Prevención y Control del Tabaquismo (PIT) 2024–2027”) includes different areas of intervention. This Plan should be followed by specific legislative changes that would contribute to improving the current and future health of the population14 with a clear impact on decreasing the prevalence of tobacco consumption and exposure to SHS, and in decreasing the incidence of cancer, respiratory and cardiovascular diseases. The consideration of SHS as a risk factor by all AC, without exception, is a necessary step. In addition, the inclusion of standardized questions to ascertain exposure to SHS in all Spanish health surveys should be mandatory.
FundingThis work has been funded by the Instituto de Salud Carlos III (ISCIII) through the Project “PI22/00727” and co-funded by the European Union.
Conflict of InterestsThe authors state that they have no conflict of interests.







