

Asbestos is the term used for a set of mineral silicates that tend to break up into fibers. Its use has been associated with numerous diseases affecting the lung and pleura in particular, all of which are characterized by their long period of latency. Asbestos, moreover, has been recognized by the WHO as a Group IA carcinogen since 1987 and its use was banned in Spain in 2002. The publication in 2013 of the 3rd edition of the specific asbestos health monitoring protocol, together with the development of new diagnostic techniques, prompted the SEPAR EROM group to sponsor publication of guidelines, which review the clinical, radiological and functional aspects of the different asbestos-related diseases. Recommendations have also been made for the diagnosis and follow-up of exposed patients. These recommendations were drawn up in accordance with the GRADE classification system.
Asbesto, también conocido en España como amianto, es el término utilizado para nombrar a un conjunto de silicatos minerales que suelen romperse en fibras. Su uso ha comportado la aparición de numerosas enfermedades, especialmente pleuropulmonares, todas ellas caracterizadas por su prolongada latencia. El asbesto es, además, un carcinógeno del grupo IA reconocido por la OMS desde 1987. En España está prohibido desde 2002. La publicación en 2013 de la 3.ª edición del protocolo de vigilancia sanitaria específica del amianto junto con la aparición de nuevas técnicas diagnósticas han motivado al grupo EROM de SEPAR a promover la elaboración de esta normativa que revisa aspectos clínicos, radiológicos y funcionales de las diferentes enfermedades relacionadas. También establece recomendaciones para el diagnóstico y seguimiento de los pacientes expuestos. Dichas recomendaciones han sido establecidas mediante sistema GRADE.
Asbestos is divided into 2 large subgroups: amphiboles and serpentines, each with its distinct physical and chemical characteristics. Serpentine fibers are characterized by their curved shape on electron microscopy, and chrysotile or white asbestos is the only member of this subgroup. The other forms are amphiboles, which are composed of straight rigid fibers of varying length, generally less than 5μm.1
Asbestos is characterized by its resistance to high temperatures and chemicals, and its high tensile strength. It is used in more than 3000 different applications in numerous industrial sectors, and even in other widely distributed products such as toys, toasters, dryers, smoking goods, etc. Asbestos comes in different forms: a) loose fill, b) sheets or plaques, c) entwined in yarn or woven into cloth, d) fiber cement, and e) as a component of mortar. These widely ranging forms often make it difficult to identify asbestos as a material used by workers when recording their employment history. In 2002, Community Directive 1999/77 came into force, banning the use of all types of asbestos in the European Union.2 Today, occupational exposure to asbestos continues to be a risk for workers involved in the demolition, maintenance, repair and transport of structures in which asbestos was previously used. In Spain, Royal Decree (RD) 396/20063 sets down all the necessary provisions for the care of these workers’ health.
Malignant and non-malignant asbestos-related diseases and their pathogenesis (in these recommendations we will use the word benign instead of non-malignant) are listed in supplementary material, available online.
Diagnostic Tests for Evaluating Asbestos-related DiseaseEmployment HistoryA full employment history must be collected (consistent recommendation, high quality of evidence). The patient must be asked about their employment, professional category, degree of protection, degree of exposure, and company medical check-ups during their working life.
If there is any known exposure to asbestos, the following data will also be collected:
- -
year of first exposure, duration and end of exposure
- -
Type of exposure: occupational, from working directly with asbestos; domestic, from building insulation or other contaminants or from washing work clothes; environmental, from the use of asbestos in public spaces, demolition of buildings, or proximity to polluting factories.
- -
Intensity. Intense exposure is considered direct contact for more than 6 months (8h a day, 40h a week) or a high concentration of asbestos fibers in the air breathed (Ministerial Order 31 October 1984. State Bulletin (BOE) 7 November 1984). The risk of exposure covers an area within a 300–2200m radius from the source depending on wind direction, and occupational exposure is generally significant after 6 months of work4 (consistent recommendation, very low quality of evidence).
- -
Type of asbestos used. Depending on profession.
- -
Concomitant smoking index.
Chest radiograph (Rx) is the basic tool for identifying asbestos-related diseases (consistent recommendation, moderate quality of evidence).
The International Labor Office (ILO) chest Rx classification is useful for systematically describing and recording radiographic abnormalities in the chest observed not only in asbestosis, but in any type of pneumoconiosis. The latest edition also reviews the criteria for classifying pleural thickening.5 These criteria, then, are useful for describing radiological abnormalities, although they are not a prerequisite for diagnosis.
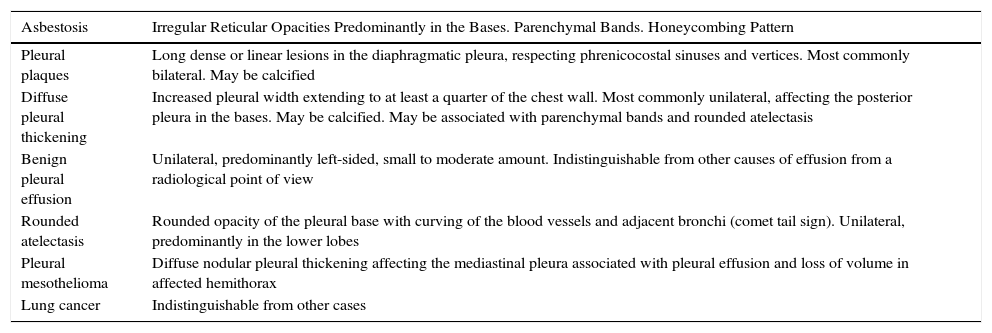
Computed tomography (CT) is a more sensitive diagnostic tool (Table 1).
Radiological Characteristics of Pleuropulmonary Asbestos-related Diseases.
| Asbestosis | Irregular Reticular Opacities Predominantly in the Bases. Parenchymal Bands. Honeycombing Pattern |
|---|---|
| Pleural plaques | Long dense or linear lesions in the diaphragmatic pleura, respecting phrenicocostal sinuses and vertices. Most commonly bilateral. May be calcified |
| Diffuse pleural thickening | Increased pleural width extending to at least a quarter of the chest wall. Most commonly unilateral, affecting the posterior pleura in the bases. May be calcified. May be associated with parenchymal bands and rounded atelectasis |
| Benign pleural effusion | Unilateral, predominantly left-sided, small to moderate amount. Indistinguishable from other causes of effusion from a radiological point of view |
| Rounded atelectasis | Rounded opacity of the pleural base with curving of the blood vessels and adjacent bronchi (comet tail sign). Unilateral, predominantly in the lower lobes |
| Pleural mesothelioma | Diffuse nodular pleural thickening affecting the mediastinal pleura associated with pleural effusion and loss of volume in affected hemithorax |
| Lung cancer | Indistinguishable from other cases |
Bénard6 demonstrated the utility of this technique for distinguishing benign pleural lesions from pleural mesothelioma, thanks to its high sensitivity, specificity, and diagnostic accuracy, in addition to its high positive predictive value, and particularly, its high negative predictive value (92%; 75%; 89%; 94.3% and 92%, respectively). Subsequent studies confirmed these findings.7 Dual PET is also helpful in the diagnostic process (the SUV index increases in the late phase compared to the early phase in mesotheliomas, and falls in benign lesions). Similar values are obtained on PET-CT. The SUV value varies among the different studies. If there is a high clinical suspicion of mesothelioma, or if PET or PET-CT is positive, the diagnosis must be confirmed with a pathology study of a pleural tissue biopsy obtained preferably by surgery (consistent recommendation, high quality of evidence).
PET-CT is also a useful imaging technique in mesothelioma staging and in the study of lesions of the pulmonary parenchyma, since, unlike in lung cancer, there is no uptake of radiotracer in rounded atelectasis. A positive result needs histological confirmation.8
Magnetic Resonance and Other Imaging TechniquesThe role of magnetic resonance imaging (MRI) in asbestos-related diseases is very limited.
It may be helpful in distinguishing malignant pleural tumors from benign lesions, based on morphological changes and signal intensity.9 In rounded atelectasis, MRI shows the visceral pleura infolding into the lesion (consistent recommendation, moderate quality of evidence).
It also defines extrapleural fat more clearly, and it is more accurate in establishing invasion of the chest wall and the diaphragm in mesothelioma staging, although it is not useful for detecting subdiaphragmatic invasion.10
Pleural ultrasonography is useful in the study of pleural effusion and peripheral masses as an imaging tool for guiding procedures such as thoracocentesis, pleural biopsy, etc. No studies are available to support its use in other asbestos-related diseases (consistent recommendation, high quality of evidence).
Lung Function TestsLung function testing is mandatory in the diagnosis and follow-up of asbestos-related diseases. When used in the context of health surveillance, it contributes to the early diagnosis of exposed individuals, and it is indispensable for evaluating a patient's capacity for work (consistent recommendation, high quality of evidence).
Spirometry is the initial procedure; forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and FEV1/FVC can be used to detect and quantify obstructive ventilatory defects, and alert to a restrictive defect. The measurement of lung volumes is mandatory for diagnosing a restrictive ventilatory defect. Measurement of diffusing capacity (DLCO) is a sensitive test, but it lacks specificity in the detection of interstitial lung disease and has a greater coefficient of variation than spirometry.11 In asbestosis, the characteristic functional change is a restrictive ventilatory pattern (reduced total lung capacity), and DLCO is usually reduced, both as a result of fibrosis of the pulmonary parenchyma. A reduced diffusing capacity is one of the most sensitive tests for early-stage asbestosis, although specificity is low. Diffuse thickening of the visceral pleura without interstitial involvement can also cause a restrictive ventilatory defect.12 After much debate, pleural plaques were not considered to be responsible for changes in lung function which, when it occurs, is due to other concomitant causes, such as onset of interstitial involvement or smoking.13
Mineralogical AnalysisAsbestos can be detected in respiratory samples on optical microscopy, in the form of asbestos bodies (AB), also known as ferruginous bodies, formed after the fibers are coated with proteic material within the macrophages. The observation of AB in standard pathology samples using routine histological staining (hematoxylin-eosin) is very specific, but sensitivity is very low. For this reason, specific processing of the samples is required for the evaluation of the pulmonary content of asbestos by AB counts in lung tissue or bronchoalveolar lavage14 (consistent recommendation, high quality of evidence). Samples of lung tissue weighing at least 0.5g are required, and these are digested in sodium hypochlorite, filtered, and washed. AB quantification is performed using a 400× optical microscope. The size of the samples required means that they are usually obtained from lobectomies, pneumonectomies, or autopsy samples. Values in pulmonary biopsy or bronchoalveolar lavage of more than 1000AB/g of dry lung tissue or 1 AB per milliliter of bronchoalveolar lavage are indicative of exposure. An electron microscope is required for detection of asbestos fibers. If the aim is to identify the chemical composition of the fiber to determine its type, various sample analysis methods are available, including energy dispersive X-ray spectroscopy. A well-equipped laboratory and trained personnel are required for these procedures, and each laboratory must establish reference values according to the local population. The first step required for validation of the laboratory in this technique is standardization, since notable differences have been found between groups in different countries. In Spain, the reference values for pulmonary AB in the unexposed population have recently been published.15 According to the values obtained, it was confirmed that the international threshold of 1000 AB is appropriate in our setting for classifying potentially disease-causing values.
BiomarkersSeveral blood and pleural fluid markers of malignant pleural mesothelioma have been studied, such as hyaluronic acid, carcinoembryonic antigen or CA 125, but none has been shown to be useful. Osteopontin is produced by malignant pleural mesothelioma, and levels in serum are directly associated with years of exposure and with the intensity of the lesions. The lack of specificity limits the diagnostic utility of this marker.
The drawback of soluble mesothelin is that it is not expressed in the sarcomatous subtype. Levels in serum and in pleural fluid correlate very closely. A recent metaanalysis studying the efficacy of soluble mesothelin in the diagnosis of malignant pleural mesothelioma concluded that for a cutoff point of 2ng/ml in plasma, the area-under-the-curve is 0.77 (95% CI: 0.73–0.81) with 95% specificity, but a very low sensitivity of 32%.16 Given the high specificity of this marker, positive values in risk populations require that the patient be examined in further depth. However, its low specificity means that a negative result does not rule out the diagnosis. Thus, the systematic determination of soluble mesothelin in the exposed population is not recommended as a method of early diagnosis (consistent recommendation, high quality of evidence).
Fibulin-3, a new biomarker described in glioma cells, is involved in tumor invasion and growth. Studies in malignant pleural mesothelioma have shown that fibulin-3 levels in plasma have 96% sensitivity and 95% specificity, and when it is found in pleural fluid, sensitivity is 84% and specificity 93%. In contrast to soluble mesothelin, there is no correlation between levels in serum and levels in pleural fluid. Levels of fibulin-3 in plasma can help distinguish individuals exposed to asbestos from patients with malignant pleural mesothelioma, and in the latter group, levels are associated with prognosis. However, soluble mesothelin has been shown to be superior to fibulin-3 as a diagnostic marker.17 Despite its low sensitivity, which makes it less useful as a method for screening the exposed population, soluble mesothelin is still the most effective biomarker for diagnosing mesothelioma (consistent recommendation, low quality of evidence).
Legislation and Specific Asbestos Health Surveillance ProtocolThe current legal framework is based on RD 1299/2006 (supplementary material, available online, Annex I). The classification of occupational diseases was updated in this RD, and a list of activities that might cause occupational disease was provided. Asbestos-related diseases are listed in Annex II (supplementary material, available online), recently expanded to include laryngeal cancer.18 Six groups of occupational diseases are specified. Exposure to asbestos appears in Group 4 (non-tumor diseases) and in Group 6 (tumor diseases).
Moreover, the law makes it mandatory for any National Health System doctor to report any disease caused by occupational exposure to one of these substances as a suspected occupational disease. A standard declaration form is available for this purpose, which is assessed by the managing body, generally the Spanish National Institute of Social Security, and either accepted or rejected. This declaration is important for subsequent litigation, and determines the period of statute of limitations, generally 1 year after rejection.
The law also demands that companies provide information, which has led to each autonomous community setting up lists of companies in which asbestos has been used.
Since this RD was enacted, only 1 regulation associated with this issue has appeared: RD 843/2011, regulating risk prevention services in the workplace.
Under this framework, the autonomous communities have set up programs for risk prevention in the workplace and assistance to exposed individuals.
Application of the Specific Health Surveillance Protocol: First Visit and Visit intervals. Recommendations of the EROM GroupArticle 16 of RD 396/2006, dated 31 March 2006, setting down the minimum provisions for health and safety applicable to jobs with risk of exposure to asbestos, states that “taking into account the long period of latency of the pathological manifestations of asbestos exposure, any worker with a history of exposure to asbestos who ceases their working relationship with the company in which the situation of exposure arose, whether due to retirement, change of company, or any other reason, will continue to undergo preventive medical check-ups, by way of regular examinations performed by the National Health System in respiratory medicine departments equipped with the appropriate resources for the examination of respiratory function, or in other departments associated with asbestos-related diseases”.
In Spain, as in other countries, a screening and surveillance program is available for workers exposed to asbestos. These are medicolegal programs that are highly important in the identification and diagnosis of the different diseases, but there is little scientific evidence that this is an effective strategy for improving the course of these diseases.
In view of this, the SEPAR EROM group recommends that the tests performed in the first and successive visits and the visit intervals should be as follows:
1) First visit of a patient consulting with a history of possible asbestos exposure:
- -
Employment history: as listed above.
- -
Smoking history: if active smoker, anti-smoking counseling or treatment (consistent recommendation, high quality of evidence).
- -
Medical history and case history: the patient will be asked particularly about respiratory symptoms (dyspnea, cough and expectoration, chest pain, hemoptysis) and asthenia, anorexia, and weight loss.
- -
Physical examination: assess for the presence of crackles and nail clubbing.
- -
Additional tests:
- -
Chest Rx.
- -
Full lung function testing with forced spirometry, lung volumes and DLCO in a laboratory equipped for functional testing, following SEPAR recommendations.
If the probability of exposure is zero or unclear from the patient's employment history (their job does not appear on the list of activities with risk of exposure to asbestos http://www.msssi.gob.es/ciudadanos/saludAmbLaboral/docs/ProtoVigiAmianto1.pdf) and test results are normal, the follow-up will terminate at this point.
An HRCT should be performed if changes are observed on the chest Rx, lung function tests are abnormal, or if a clinical/functional discrepancy is observed (consistent recommendations, low quality of evidence).
While it is true that CT is more sensitive than chest Rx for the diagnosis of uncalcified pleural plaques, its use for diagnosis in a patient with a normal chest Rx, normal functional tests and no symptoms is questionable and not supported by scientific evidence (the risk-benefit ratio due to radiation must also be taken into account).
Another issue is the use of CT as a screening tool for lung cancer in early disease stages. In this respect, a metaanalysis recently published in Chest19 of over 5000 workers in total found a prevalence of lung cancer in individuals exposed to asbestos of 1.1%, similar to that reported in the study on lung cancer screening in heavy smokers (1%: 95% CI: 0.09–1.1%).20 For this reason, the study concludes that CT screening in workers exposed to asbestos may be effective for detecting asymptomatic, early-stage lung cancer, so it may reduce lung cancer mortality in this group of workers.
Lung cancer screening among workers exposed to asbestos is an urgent matter that requires a large, randomized trial to establish consistent recommendations based on high-quality scientific evidence.
2) Regular visits will take place at the established intervals, depending on the diagnostic findings, and provided the patient is asymptomatic and shows no changes in symptoms (consistent recommendation, low quality of evidence):
- -
No disease: check-up with forced spirometry and chest Rx every 3 years.
- -
Pleural disease with pleural plaques: check-up every 1–3 years with chest Rx and forced spirometry. If pathological, complete the study with full lung function testing including volumes and DLCO.
- -
Pleural disease with diffuse pleural thickening: annual check-up with chest Rx and full functional study with volumes and DLCO.
- -
Pleural disease due to asbestos with rounded atelectasis: if typical radiological signs are observed, monitor stability over time with imaging techniques, preferably CT every 6 months for 2 years. Subsequent follow-up similar to that of diffuse pleural thickening (consistent recommendation, low quality of evidence). In the absence of typical radiological signs or if symptoms are observed, consider other techniques (PET, PET-CT, CT-guided FNAB) to rule out malignancy (consistent recommendation, high quality of evidence).
- -
Asbestosis: annual check-up with chest Rx and full functional study. In case of deteriorating lung function tests or radiological changes on chest Rx, consider repeating high-resolution CT.
- -
Anti-smoking treatment if patient continues to smoke.
Changes in symptoms, in lung function tests, or in radiological studies may call for a repeat CT.
Neither determination of biomarkers nor regular CTs are currently indicated for the early detection of mesothelioma (Fig. 1).
Criteria for Attributing Diseases to Asbestos
Attributing a disease to asbestos has a diagnostic significance that will affect subsequent monitoring and may also have legal and economic implications, since mesothelioma, asbestosis, lung cancer, and pleural fibrosis associated with ventilatory restriction are recognized as occupational diseases. The fact that asbestos can cause a whole series of respiratory diseases does not make attribution any easier in each specific case. This is because the available epidemiological and experimental data show that exposure must meet certain criteria in terms of intensity and duration in order to be considered a causative factor for a specific disease.
As in other diseases caused by inhalation of substances, the diagnosis of processes caused by asbestos require exposure, consistent clinical and radiological picture, and the exclusion of any other reasonable cause. Thus, the diagnosis of mesothelioma usually involves attribution to asbestos, since no other agent that clearly causes the disease has been identified, and benign pleural diseases display radiological signs that can make them easier to recognize.
As a general rule, the characteristics of the exposure must be evaluated. Asbestosis is unlikely to develop with accumulated exposures lower than 25 fibers/ml/year,21 and the increase in the incidence of lung cancer also occurs after intense exposures for period of longer than 20 years. In contrast, benign pleural diseases can appear after 10 years from first exposure, and exposure can be of mild intensity.
In practice, the patient is not usually aware of the concentration of fibers present in the work environment, and it may be difficult for the doctor to evaluate the intensity of exposure from the information obtained from the employment history. Indeed, even with the use of a comprehensive questionnaire, sensitivity and specificity for detecting exposure are only 50% and 75%, respectively, with respect to the number of ABs detected in lung tissue (personal unpublished data). In the case of domestic or environmental exposure, it is more difficult to establish the causal relationship.
In patients with a known history of exposure, associated diseases may be attributed to that exposure without other considerations (consistent recommendation, moderate quality of evidence).
If, however, discrepancies are detected between the clinical picture or imaging tests and the notion of exposure, it is useful to have objective evidence of exposure. The gold standard is the detection of asbestos in the lung, determined by testing for AB (deposits in the pleura are generally scant). Values indicative of pulmonary deposits liable to cause disease are 103AB/g in dry lung or more than 106fibers/g, according to data from the only laboratory is Spain that has reference values.15 This technique can also be carried out in bronchoalveolar lavage, with threshold values of 1AB/ml.
The appearance of new fibers that have replaced asbestos and their possible impact on health are reviewed in supplementary material, available online.
Conflict of InterestsThe authors state that they have no conflict of interests.
The following are the supplementary data to this article:
Please cite this article as: Roza CD, Cruz Carmona MJ, Álvarez RF, Sancho JF, Martínez BM, González CM, et al. Recomendaciones sobre el diagnóstico y manejo de la enfermedad pleural y pulmonar por asbesto. Arch Bronconeumol. 2017;53:437–442.







