


We report the case of a 30-year-old patient, diagnosed in 2011 with vascular Ehlers-Danlos syndrome (also called Ehlers-Danlos syndrome type IV), who had presented several episodes of bilateral pneumothorax in the previous 2 years. Although the most significant complications presented by this patient were associated with the formation and spontaneous rupture of aneurysms in multiple arteries (carotid, renal, splenic, vertebral, etc.), since 2013 a wide variety of pulmonary nodules had also appeared on incidental radiological images, including solid nodules (Fig. 1A), subsolid nodules (Fig. 1B), cavitary nodules (Fig. 1C), and nodules containing calcifications (Fig. 1D).
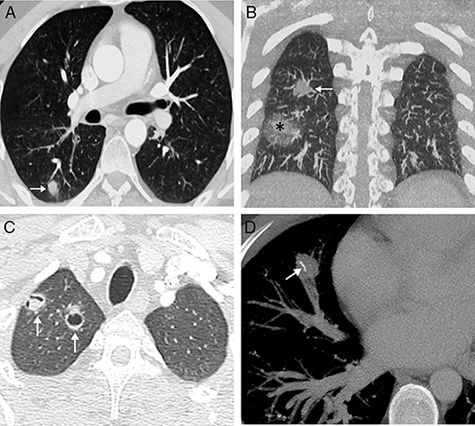
(A) Chest CT axial image (pulmonary parenchymal window) from 2013, showing a solid nodule in the right lower lobe (arrow). (B) Chest CT coronal image of the scan of the (pulmonary parenchymal window) from 2014, showing the appearance of 2 nodules in the right lung: one solid (arrow) and other subsolid with mainly ground glass attenuation and a small, solid core (asterisk). (C) Chest CT axial image (pulmonary parenchymal window) from 2016 showing the appearance of 2 cavitary lung nodules in the right pulmonary apex (arrows). Note that the most lateral nodule has non-centered cavitation with half-moon morphology. (D) Chest CT axial image (mediastinal window) from 2017 in which linear calcification (arrow) has appeared within a solid nodule in the middle lobe.
Ehlers-Danlos syndrome is a rare autosomal dominant connective tissue disorder, in which a COL3A1 gene mutation causes abnormal type III procollagen synthesis, increasing the likelihood of spontaneous rupture of arteries and vital organs. Very few references are available on the pulmonary radiological manifestations of this rare syndrome, but they seem to be triggered by the spontaneous formation of lung lacerations (caused by systemic tissue fragility), which may progress to bruising, cavitary nodules, fibrous nodules, and finally nodules with metaplastic ossification.1,2 In the absence of clinical evidence of infection (as in our case), it is reasonable to attribute the etiology of the pulmonary nodules to inherent tissue fragility causing the spontaneous formation of parenchymal lacerations, and to progressive secondary changes in the lung tissue, as described by some authors.2
Please cite this article as: Gorospe Sarasúa L, Muñoz-Molina GM, Arrieta P. Las muchas caras radiológicas de los nódulos pulmonares en el síndrome de Ehlers-Danlos tipo iv. Arch Bronconeumol. 2018;54:626.







