


La supervivencia del trasplante pulmonar (TP) viene condicionada fundamentalmente por el desarrollo de disfunción crónica del injerto (DCI). El retrasplante pulmonar (RP) es una alternativa para una población seleccionada con DCI. El objetivo del estudio fue revisar la experiencia de RP en nuestro centro.
Pacientes y métodosSe ha realizado un estudio retrospectivo de los pacientes sometidos a RP entre agosto de 1990 y julio de 2017.
ResultadosSe realizaron 14 RP de un total de 998 (1,4%) TP. Doce RP se dieron por causa de DCI: 10 (71,4%) por síndrome de bronquiolitis obliterante y 2 (14,3%) por síndrome restrictivo del injerto. En 2 pacientes el RP se realizó en los 30 días siguientes al primer TP. En el RP por DCI el tiempo medio entre el TP y el RP fue de 48 meses. Tras el RP el tiempo medio de ventilación mecánica fue de 32 días. El incremento del FEV1 tras el RP fue del 24±18%. Los mejores valores en la espirometría se observaron a los 7,3 meses. La supervivencia media de la serie fue de 43,8 meses, en los pacientes con síndrome de bronquiolitis obliterante fue de 63,4 meses mientras que en los pacientes con síndrome restrictivo del injerto fue de 19,5 meses. Solo un paciente de los 2 RP precoces sobrevivió a este.
ConclusiónEl RP es una opción terapéutica en pacientes seleccionados con DCI. Sin embargo, estos resultados no son reproducibles si el RP se realiza en los primeros días.
Long-term survival of lung transplantation (LT) patients is mainly limited by the development of chronic lung allograft dysfunction (CLAD). Lung retransplantation (LR) is an alternative for a selected population. The aim of this study was to review the LR experience in our center.
Patients and methodsWe conducted a retrospective study of patients undergoing LR between August 1990 and July 2017.
ResultsFourteen LR out of a total of 998 (1.4%) LT were performed. Twelve patients (85.7%) underwent LR due to CLAD: 10 (71.4%) because of bronchiolitis obliterans syndrome and 2 (14.3%) due to restrictive allograft syndrome. LR was performed in 2 patients within 30 days of the first LT. In those who underwent LR due to CLAD, mean time between the first LT and LR was 48 months, and mean duration of invasive mechanical ventilation was 32 days. The increase in FEV1 after LR was 24±18%. The best spirometry values were observed after 7.3 months. Mean survival of the cohort was 43.8 months. In patients with bronchiolitis obliterans syndrome, mean survival was 63.4 months, while in those with restrictive allograft syndrome, it was 19.5 months. Only 1 of the 2 early LR patients survived.
ConclusionLR is a therapeutic option in selected patients with CLAD, with acceptable survival. Indication for LR early after LT shows poor outcomes.
El trasplante pulmonar (TP) es el tratamiento de elección en pacientes seleccionados con enfermedad respiratoria irreversible cuando el tratamiento médico no ha sido eficaz. Desde hace 2 décadas el TP se considera el mejor tratamiento en estos pacientes para alargar y mejorar la calidad de vida, así como la capacidad de esfuerzo1. Pese a los avances obtenidos en el tratamiento de estos pacientes, la supervivencia continúa siendo inferior a la de otros trasplantes de órganos sólidos2. Según datos del Registro Internacional de Trasplante de Corazón y Pulmón (RIHLT), en el intervalo de enero 1990 a junio 2012 la supervivencia media fue de 5,7 años3. El TP presenta peculiaridades que condicionan su supervivencia y que lo hacen diferente a otros trasplantes de órganos sólidos. De entre estas destacan el hecho de que sea un órgano con exposición constante al medio externo, ya que facilita las infecciones y los efectos de la contaminación4, las microaspiraciones, el reflujo gastroesofágico o el abundante tejido linfoide5. Todos estos factores se consideran de riesgo para el desarrollo de disfunción crónica del injerto (DCI), que es la causa fundamental de pérdida del injerto a largo plazo.
Se entiende por DCI el deterioro progresivo de la función pulmonar tras el trasplante que es debido a un proceso intrínseco pulmonar6. Dentro de la DCI, diferenciamos el síndrome de bronquiolitis obliterante (BOS) definido por la presencia de obstrucción persistente y crónica con una pérdida superior al 20% del FEV1 que ocurre en 3 cuartas partes de los pacientes que desarrollan una DCI progresiva. En 2011 Sato et al. describieron un nuevo fenotipo que recibió el nombre de síndrome restrictivo del injerto (RAS)7,8. El RAS se caracteriza por una caída funcional del FEV1 de al menos un 20% respecto al mejor CVF o bien una pérdida>10% de la TLC. Estos pacientes presentan además hallazgos radiológicos en forma de infiltrados pulmonares no explicables por otras causas, así como cambios histológicos como daño alveolar difuso o fibrosis. Existe un porcentaje no despreciable de pacientes en los que conviven ambos fenotipos, sin embargo, no están bien definidos estos casos mixtos y generalmente se suelen clasificar como RAS.
El desarrollo de un fenotipo u otro tiene especial relevancia clínica dado que el pronóstico vital tras el diagnóstico es diferente entre ambos. De tal forma que los pacientes con RAS presentan un curso clínico más rápido con una supervivencia media tras el diagnóstico de solo 1,5 años frente los 4 años de aquellos que son diagnosticados de BOS9. En líneas generales el tratamiento médico de estas 2 condiciones ha presentado resultados pobres y, por lo tanto, no es de extrañar el creciente interés por ofrecer al paciente una segunda oportunidad a través de un segundo trasplante. De hecho, el retrasplante pulmonar (RP) en pacientes seleccionados es el único tratamiento que ha mostrado tener un impacto sobre la supervivencia10–12. Según datos del RIHLT, entre enero de 1995 y junio de 2013, el 5,1% de trasplantes unilaterales y el 3,4% de trasplantes bilaterales fueron retrasplantes, siendo el BOS la indicación más frecuente3. En el presente estudio se revisa la serie de pacientes retrasplantados desde el inicio del programa de TP en nuestro centro.
Pacientes y métodosSe revisaron retrospectivamente los datos de los pacientes a los que se les realizó un RP en nuestro centro desde el 1 de agosto de 1990 al 31 de julio de 2017. Las enfermedades más frecuentes fueron la enfermedad pulmonar obstructiva crónica, la enfermedad pulmonar intersticial y las bronquiectasias/fibrosis quística. Fueron considerados potenciales candidatos a un RP aquellos que cumplieron los criterios establecidos en el consenso de selección de candidatos a TP13.
En los pacientes que presentan una mala evolución de un TP se considera de forma rutinaria las probabilidades de RP. En todos los casos se toma una decisión de consenso por parte del comité de TP del centro. Para la indicación del RP se consideraron factores como las dificultades quirúrgicas potenciales, los aislamientos microbiológicos, el estado general del paciente, la fragilidad y la función del resto de los órganos.
Este estudio analiza de forma retrospectiva los resultados de todos los retrasplantes pulmonares realizados desde el inicio del programa de TP mediante la revisión sistemática de sus historias clínicas. Se analizaron las siguientes variables: indicación de RP, tratamiento inmunosupresor, evolución espirométrica, días de estancia en unidad de cuidados intensivos (UCI) y en el hospital, tiempo de ventilación mecánica, complicaciones microbiológicas e inmunológicas, mortalidad y sus causas.
Para el estudio descriptivo las variables cuantitativas se presentan como media, desviación estándar y rango. Las variables cualitativas se expresan como frecuencia y porcentaje. Para los cálculos de la supervivencia se utilizó el método de Kaplan-Meier.
ResultadosDesde agosto de 1990 a julio de 2017 se realizaron 14 RP que representa el 1,4% del total de los 998 TP realizados en este período. De ellos, 10 (71,4%) pacientes fueron mujeres y 4 (28,6%) hombres. La edad media en el momento del RP fue de 31,7 años (rango 17,6-49,5). Las características y complicaciones de la población tras el primer trasplante y el RP se describen en la tabla 1.
Complicaciones pacientes RP
| S | Dx inicial | TP | Motivo RP | RP | Comorbilidades preRP | Edad al RP | Días estancia UCI | Tiempo VMI | DCI RP | Fecha exitus | Causa exitus | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DM | IR | |||||||||||
| M | FPI | 1990 TUPI | DCI | 1993 TUPD | No | No | 23 | - | - | No | 1993 | Complicaciones secundarias a IQ |
| M | FQ | 1997 BP | DCI | 2017 BP | Sí | Sí | 42 | 10 | 4 | No | No | |
| H | EPOC | 1998 TUPI | Complicación quirúrgica | 1998 TUPI | No | No | 49 | 37 | 33 | No | 1998 | Fallo multiorgánico |
| M | FQ | 1999 BP | DCI | 2001 TUPI | No | No | 17 | 7 | 7 | No | 2001 | Shock hemorrágico |
| M | FPI | 2005 BP | DCI | 2011 TUPD | No | No | 15 | 9 | 7 | BOS | 2017 | Hemoptisis masiva |
| H | FQ | 2006 BP | DCI | 2009 TUPD | Sí | Sí | 31 | 89 | 86 | No | 2011 | Aspergilosis pulmonar |
| M | HX | 2007 BP | DCI | 2010 TUPD | No | No | 32 | 41 | 36 | BOS | No | |
| H | FQ | 2009 BP | DCI | 2013 BP | No | No | 18 | 36 | 34 | No | No | |
| M | FQ | 2009 BP | DCI | 2016 TUPI | Sí | Sí | 33 | 20 | 12 | No | No | |
| H | FQ | 2010 BP | DCI | 2014 BP | No | No | 19 | 47 | 36 | No | No | |
| M | NH | 2012 TUPI | Complicación quirúrgica | 2012 TUPI | No | No | 57 | 24 | 17 | BOS | No | |
| M | NINE | 2013 BP | DCI | 2015 TUPD | Sí | Sí | 51 | 37 | 31 | RAS | 2016 | Neumonía |
| M | BO | 2013 BP | DCI | 2015 BP | No | No | 3 | 94 | 94 | No | 2015 | Aspergilosis pulmonar angioinvasiva |
| M | EPOC | 2013 BP | DCI | 2016 BP | No | No | 54 | 33 | 22 | No | No | |
BO: bronquitis obliterante; BP: bipulmonar; DCI: disfunción crónica del injerto; DM: diabetes mellitus; Dx: diagnóstico; EPOC: enfermedad pulmonar obstructiva crónica; FPI: fibrosis pulmonar idiopática; FQ: fibrosis quística; H: hombre; HX: histiocitosis X; IQ: intervención quirúrgica; IR: insuficiencia renal; M: mujer; NH: neumonitis por hipersensibilidad; RAS: síndrome restrictivo del injerto; RP: retrasplante pulmonar; S: sexo; TP: trasplante pulmonar; TUPD: trasplante unipulmonar derecho; TUPI: trasplante unipulmonar izquierdo; UCI: unidad de cuidados intensivos; VMI: ventilación mecánica invasiva.
El RP se indicó en 12 (85,7%) pacientes por DCI; 10 (71,4%) en forma de BOS y 2 (14,3%) en forma de RAS. En los 2 casos restantes el RP se indicó por complicaciones quirúrgicas que se produjeron en el postoperatorio inmediato.
En los 12 pacientes con DCI, en el momento del RP la función pulmonar media en el caso de la FVC fue del 49,6±14,2% y del FEV1, del 34,8±11,7%. El tiempo medio entre el primer TP y el RP fue de 48±58,2 meses. Se realizaron 5 (35,7%) RP bilaterales, 4 (28,6%) RP unilaterales izquierdos y 5 (35,7%) derechos.
El protocolo de inmunosupresión inicial consistió en un inhibidor de la calcineurina (tacrolimus), un inhibidor de la síntesis de purinas principalmente micofenolato mofetil, aunque en un caso se utilizó azatioprina, y en todos los casos metilprednisolona. En 5 (35,7%) pacientes se administró basiliximab: 2 de ellos eran TP infantiles utilizándose como terapia de inducción mientras que en el caso de los 3 TP de adultos se utilizó en el postoperatorio inmediato por presentar insuficiencia renal (IR) que impedía la introducción de anticalcineurínicos.
La estancia hospitalaria media tras el RP fue de 48±29 días, el tiempo medio en la UCI fue de 37±28 días y el tiempo medio de ventilación mecánica invasiva fue de 32±29 días.
El mejor funcionalismo se alcanzó a los 7,3±9,9 meses del RP con un incremento del FEV1 tras el RP de 24±18% y de la FVC de 59,4±15,8% respecto al basal con un FEV1 medio de 58±17,4%.
Complicaciones perioperatoriasLa mortalidad perioperatoria fue de 3 (21,4%) pacientes. Uno falleció a las 24h por complicaciones secundarias a la intervención quirúrgica. Otro a los 8 días por desgarro de la arteria pulmonar a nivel de la anastomosis que le ocasionó un shock hemorrágico. El último no pudo salir de circulación extracorpórea y requirió oxigenación por membrana extracorpórea, siendo exitus a los 18 días por sangrado recidivante que incluso requirió neumonectomía izquierda. En la autopsia se observó aspergilosis pulmonar angioinvasiva.
Presentaron disfunción primaria del injerto 3 (21,4%) pacientes, 2 de ellos de grado iii y uno de grado i.
Complicaciones tardíasDesde el 30.o día postrasplante hasta la finalización del estudio, la mortalidad fue de 4 (28,6%) pacientes. Las principales causas fueron infecciosas en 3 casos y una hemoptisis masiva. Durante este período, 3 (21,4%) pacientes padecieron infecciones fúngicas: 2 (14,3%) por Aspergillus fumigatus en forma de traqueobronquitis y una (7,1%) por Aspergilus niger en forma de aspergilosis pulmonar cavitada. Dos (14,3%) pacientes presentaron replicación de citomegalovirus que requirió tratamiento con valganciclovir. Cinco (35,7%) pacientes presentaron colonización por bacterias multirresistentes: 4 (28,6%) de ellos por Pseudomonas aeruginosa y uno (7,1%) por Burkholderia multivorans. En lo referente a las suturas bronquiales, únicamente un paciente presentó estenosis en bronquio intermediario del 15% que no requirió ninguna actuación específica.
Rechazo agudo celular y crónicoLa incidencia de rechazo agudo celular demostrado por biopsia fue del 14,3%, lo cual supone 2 pacientes, uno con estadio A1 y otro A2. En ambos casos los pacientes se recuperaron y solamente se trató el de mayor grado.
Se diagnosticó de DCI a 4 (28,6%) pacientes: 3 tipo BOS y uno tipo RAS con un tiempo medio desde el RP al diagnóstico de 30±19,6 meses y una función pulmonar media en el momento del diagnóstico de FVC 37,1±15,5% y FEV1 28,3±9,3%. Los inhibidores de la mTOR se utilizaron como segunda línea de tratamiento y fueron indicados en substitución de micofenolato en 3 (21,4%) pacientes debido a recurrencia de DCI, 2 (14,3%) de ellos con rapamicina y uno (7,1%) con everolimus.
SupervivenciaLa supervivencia media tras el RP fue de 43,8±10,3 meses con una mediana de 74±36,9 meses. Excluyendo los 3 (21,4%) pacientes que fueron exitus en el período postoperatorio, la supervivencia media fue de 55,8±10,6 meses con una mediana de 74±39,5 meses.
La supervivencia media según el tipo de DCI es de 63,4±12,4 meses con una mediana de 74±40,5 meses en los pacientes con BOS, mientras que los pacientes con RAS presentaron una supervivencia media de 19,5±9,5 meses con una mediana de 6 meses.
DiscusiónLa DCI sigue siendo la principal limitación de supervivencia tras el TP, ocurriendo en el 50% de los pacientes a 5 años del procedimiento y representando alrededor del 30% de la mortalidad entre 3 y 5 años después del TP3,7. Hasta la fecha no existe un tratamiento específico para la DCI. Sin embargo, el RP en pacientes seleccionados puede alargar la supervivencia. Existen pocos estudios publicados al respecto y todos son series de casos. Este hecho probablemente se deba a la evolución que los criterios e indicación de TP han sufrido a lo largo de estos años. Por ejemplo, el consenso publicado en 1998 no consideraba la opción del RP14; fue en el consenso de 200615 donde aparece una primera mención aunque no será hasta el 2015 cuando se hable del RP específicamente. El objetivo del presente estudio fue analizar los resultados en términos de supervivencia del RP en nuestro medio.
Según datos del RIHLT, los RP que se realizaron entre enero 1990 y junio 2012 tuvieron una supervivencia media de 2,5 años. En nuestra serie la supervivencia media fue de 3,7 años, cifra claramente inferior a la que se obtiene tras un primer TP. Sea como fuere, los resultados de un segundo TP son siempre inferiores a los obtenidos en el primer TP. La selección de pacientes para un retrasplante pulmonar sigue los criterios de la ISHLT mismos que para un primer TP. Además las decisiones que se llevan a cabo se toman a través del consenso de todo el equipo multidisciplinar que busca mantener el principio de beneficencia y de igualdad de oportunidades para todos los pacientes.
Un dato a tener en cuenta es que la supervivencia observada tras el RP es superior en aquellos en los que se realiza más allá del primer año del TP. Además, otro dato relevante de este estudio es que la supervivencia observada tras el RP si este se hace por BOS es superior que si se hace por RAS. Cuando se analiza la supervivencia de los pacientes RP que sobrevivieron más allá de 3 meses al procedimiento, la supervivencia media fue de 63 meses en los pacientes que se retrasplantaron por BOS frente a los 20 meses para los que lo hicieron por RAS. Estos datos se encuentran en consonancia con datos previos publicados16. El grupo de Lovaina en un estudio descriptivo observó en los pacientes RP por RAS una supervivencia de 1,7 años frente a los 5,1 años de los RP por BOS. Existen otros estudios que analizan la supervivencia de un segundo TP, como el de Thomas et al.17 donde se describen supervivencias medias de 2,6 años o la de Novick et al.18 donde la supervivencia media tras el segundo trasplante fue de 2,5 años. Sin embargo, ambos estudios se realizaron previa descripción del fenotipo de RAS por lo que probablemente no se encontraran bien definidos ambos fenotipos en el momento de la publicación de los mismos. Dada la escasez de los estudios publicados, no son bien conocidos los factores de riesgo que justifiquen las diferencias observadas en términos de supervivencia entre ambos fenotipos. Se podría especular que la razón de una peor supervivencia en los pacientes afectos de RAS sea la presencia de un componente fibrótico y por lo tanto una mayor adherencia pleural que añade mayor dificultad al acto quirúrgico. Asimismo, la mayor necesidad de uso de sistemas de circulación extracorpórea en este subgrupo de pacientes junto con una mayor mortalidad perioperatoria por sangrado y un incremento en el número de reintervenciones tendría un impacto en la supervivencia del injerto a largo plazo.
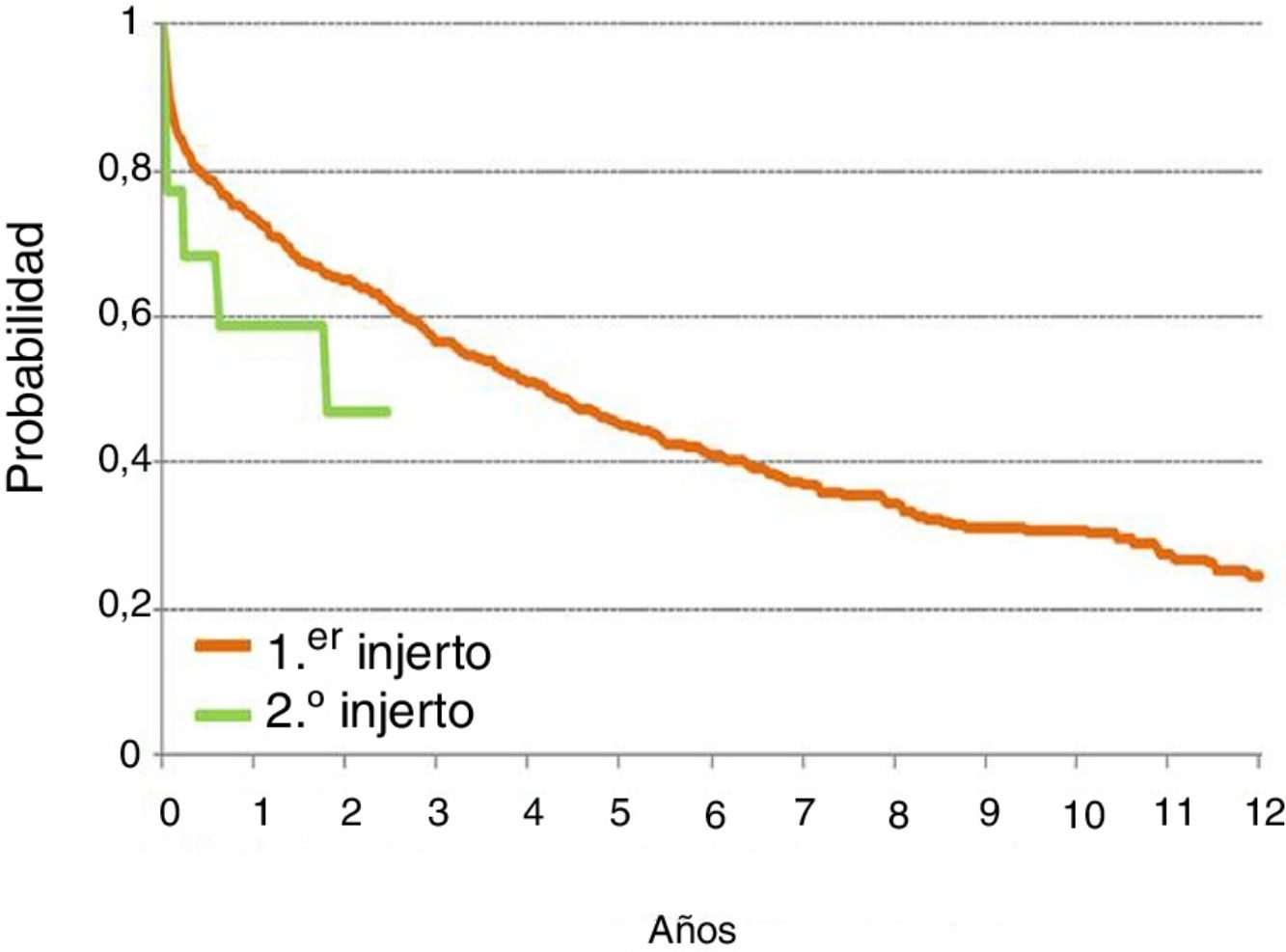
En nuestra serie la supervivencia de un primer TP respecto al RP es mejor siendo la supervivencia total al año tras un primer TP del 73% frente al 58% de los pacientes sometidos a un RP. Ver la figura resumen. Dado el pequeño número de pacientes no es posible realizar un análisis por subgrupos diferenciando los RP unipulmonares de los bipulmonares; los hallazgos encontrados con una mayor mortalidad en los casos de los unipulmonares se podría explicar por la dificultad para la extracción e implante por existencia de adherencias y también porque estos pacientes tenían una edad más avanzada respecto a los bipulmonares.
Otro dato a destacar de este estudio es que los pacientes que sobrevivieron al postoperatorio alcanzan supervivencias superiores a cualquiera de las otras estrategias terapéuticas que existen en la actualidad para tratar la disfunción del injerto, alargando la supervivencia esperada tras el diagnóstico de DCI.
De entre las causas de mortalidad perioperatoria descritas en nuestra serie se encuentran las relacionadas con el propio acto quirúrgico. Estos datos se encuentran en consonancia con los publicados por el RIHLT donde las principales causas de mortalidad perioperatoria incluyen la disfunción primaria del injerto, las infecciones no asociadas a citomegalovirus, las relacionadas con la técnica quirúrgica y las causas cardiovasculares. Estos últimos factores no se observaron en nuestra serie por tratarse de una población joven.
El tiempo medio en UCI y el de VMI es superior (37 y 32 días respectivamente) en nuestra serie de RP si lo comparamos con otras series de un primer TP como la de Riera et al. realizada en el mismo centro19. Analizaron a 100 pacientes trasplantados entre setiembre 2011 y mayo 2013 con una estancia en UCI y un tiempo de VMI medio de 21 y 15 días respectivamente.
Las comorbilidades más frecuentes que encontramos fueron la diabetes mellitus (DM) y la IR. En 6 (42,9%) de los pacientes que se sometieron a un RP, la existencia de DM fue la comorbilidad previa más frecuente. La IR definida por un filtrado glomerular menor a 60ml/min/m2 se encontró en 4 (28,6%) pacientes. Estos datos se encuentran en consonancia con los previos publicados. El grupo de Lovaina encontró que un 23% presentaba IR y un 51% tenía DM. Estos datos no fueron diferentes cuando se compararon con los pacientes con RAS (22% con IR y 34% con DM).
En cuanto a las complicaciones a largo plazo registradas en nuestros pacientes, las más comunes fueron las complicaciones infecciosas. Cinco (36%) pacientes se encontraban colonizados por bacterias multirresistentes, 2 presentaron infecciones fúngicas y en 2 pacientes existió replicación de citomegalovirus que requirió tratamiento.
Las causas inmunológicas representaron la segunda complicación en frecuencia en nuestra serie. Tres (21,4%) pacientes presentaron rechazo agudo celular que se trató con ajuste de dosis de corticoides y 4 (28,6%) pacientes desarrollaron de nuevo DCI, de estos un caso de forma precoz antes del año. Estos datos se encuentran en consonancia con los descritos en el RIHLT donde se observa que el 53,4% de los pacientes retrasplantados desarrollaran BOS a los 5 años. Se podría hipotetizar que desde un punto de vista inmunológico se trata de un grupo de población con mayor predisposición al rechazo agudo celular. Por lo que más estudios deberían realizarse para conocer todos los factores de riesgo potenciales y así evitarlos.
Probablemente uno de los factores que más impacto tenga en los resultados de supervivencia tras un RP sea el estado del receptor tal y como sucede para un primer TP. En este sentido, Novick et al.18 describen mejores supervivencias al año en pacientes ambulatorios respecto a los pacientes ingresados y con soporte ventilatorio. Por lo tanto, el RP que se realiza de forma electiva presenta mejores resultados tal como ocurre cuando se realiza un primer TP.
Este estudio presenta limitaciones al tratarse de un estudio retrospectivo basado en la experiencia de un solo centro. Sin embargo, es el primero en describir la experiencia en un centro trasplantador con gran actividad en nuestro medio. Son necesarios más estudios basados en descripción de series y experiencia clínica que permitan establecer la eficacia del RP en población susceptible de beneficiarse del mismo y definir las características de una población seleccionada que garantice buenos resultados en términos de supervivencia y buena función del injerto. Otro dato a considerar a pesar del tamaño muestral es que los pacientes sometidos a RP por RAS presentan peores resultados. Sin embargo la ausencia de un tratamiento específico para la DCI hace que el RP sea a día de hoy la única alternativa real para población seleccionada con impacto en la supervivencia. Sin duda, más estudios han de llevarse a cabo para conocer los motivos de este hecho.
Conflicto de interesesLos autores declaran no tener ningún conflicto de intereses.







