

Ulcerative colitis (UC) is an intestinal inflammatory disease occasionally associated with extraintestinal complications. We report here an atypical case of pulmonary manifestations of UC.
A 70-year-old man with a history of UC, stable in the last 5 years, receiving azathioprine, presented with a clinical picture of hemoptysis. Chest computed tomography (CT) was performed, revealing an 18-mm cavitated nodule in the right lower lobe. One month later, PET–CT was performed, showing nodule growth (19.5mm) and hypermetabolism (SUV 5.77). Bronchoscopy was normal and lung function testing found mild, non-obstructive changes (FEV1/FVC 77, FEV1 [L] 2.22 [68%], FVC [l] 2.89 [65%]). Microbiology testing of endoscopy specimens, including auramine staining and Mycobacterium tuberculosis complex DNA detection, were negative. Four weeks later, the patient had another episode of hemoptysis and respiratory failure (pO2 52mmHg). Repeat chest CT showed a 7-cm mass in the right upper lobe (RUL) (Fig. 1A). Pulmonary thromboembolism was ruled out by the contrast study. Bronchoscopy was repeated, and was normal again, and cytology and microbiology results remained negative (direct detection and bacterial, fungal and mycobacterial cultures). Pulmonary abscess was suspected, so treatment began with clindamycin with good clinical response. However, the 3-month follow-up chest CT showed that while the 7-mm RUL lesion had resolved, a new cavitated nodule had appeared in the RUL (Fig. 1B). To rule out the association with the patient's gastrointestinal disease, colonoscopy was performed, showing mild UC. The immunological examination (including antinuclear and anti-neutrophil cytoplasmic antibodies) was negative.
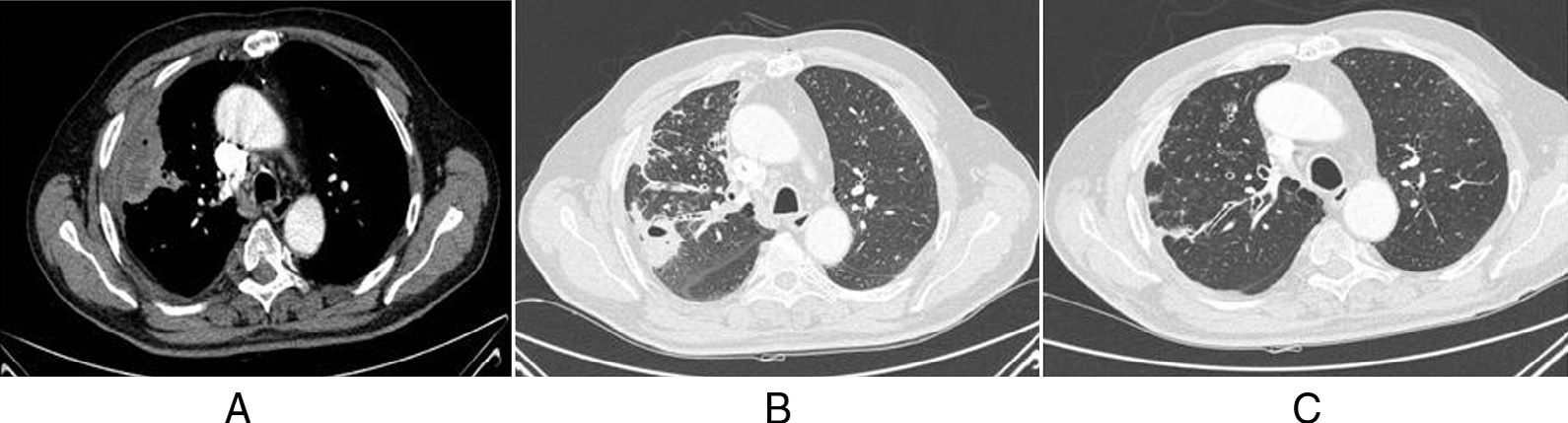
(A) Pulmonary mass in the peripheral right upper lobe (RUL) of necrotic and abscessed appearance, containing a small air bubble (mediastinal window CT image). (B) Previously described nodule has disappeared, and a new cavitated nodule has appeared close by. Bronchial wall thickening and RUL bronchial impaction (lung window CT image). (C) Resolution of previous findings (follow-up lung window CT image).
In an attempt to determine diagnosis, pulmonary biopsy by thoracotomy was performed. Pathology laboratory reports showed sterile aggregates of neutrophils with areas of necrosis and foci of organizing pneumonia, with no evidence of vascular infiltration. These findings were thought to be indicative of UC lung involvement. Treatment began with prednisone 30mg every 12h for 2 weeks, with complete resolution of radiological signs (Fig. 1C).
UC is an inflammatory disease that affects the mucosa of the colon. It manifests mainly as diarrhea, abdominal pain and rectal bleeding.1 However, in 10%–30% of cases, it can be associated with extraintestinal manifestations, particularly in the joints, skin and eyes. Pulmonary manifestations of UC are rare, multiple and non-specific.2,3 The most common symptoms are cough and wheezing.3 Our patient presented hemoptysis and respiratory failure, unusual in the published cases.2–4 Radiological findings also vary widely. The most common include bronchiectasis and ground-glass opacities.3 In our case, migratory cavitated pulmonary nodules were detected on CT, described elsewhere as very unusual.5 The most common histopathological changes are airway inflammation and bronchiectasis.2 Our patient's lung biopsy revealed foci of organizing pneumonia and necrobiotic nodules. These necrotic areas, seen on CT as abscesses, appeared sporadically during our patient's clinical course. To date, flare-ups of organizing pneumonia associated with UC have been described,4 but necrobiotic nodules are rarer.2 Treatment of UC lung involvement is based on corticosteroids.2 Our patient's response to corticosteroids was excellent, with complete clinical and radiological resolution after 2 weeks of treatment.
To conclude, this is a case of pulmonary involvement of UC, with an interesting presentation, due to exacerbations occurring with hemoptysis, respiratory failure and radiological images of migratory cavitated pulmonary nodules, with no associated clinical symptoms. Definitive diagnosis was based on lung biopsy results and response to steroid treatment was complete.
Conflict of InterestsThe authors state that they have no direct or indirect conflict of interests with the contents of this manuscript.
Please cite this article as: Barril S, Rodrigo-Troyano A, Giménez A, Sibila O. Nódulos pulmonares migratorios en paciente con colitis ulcerosa. Arch Bronconeumol. 2015;51:303-304.







