



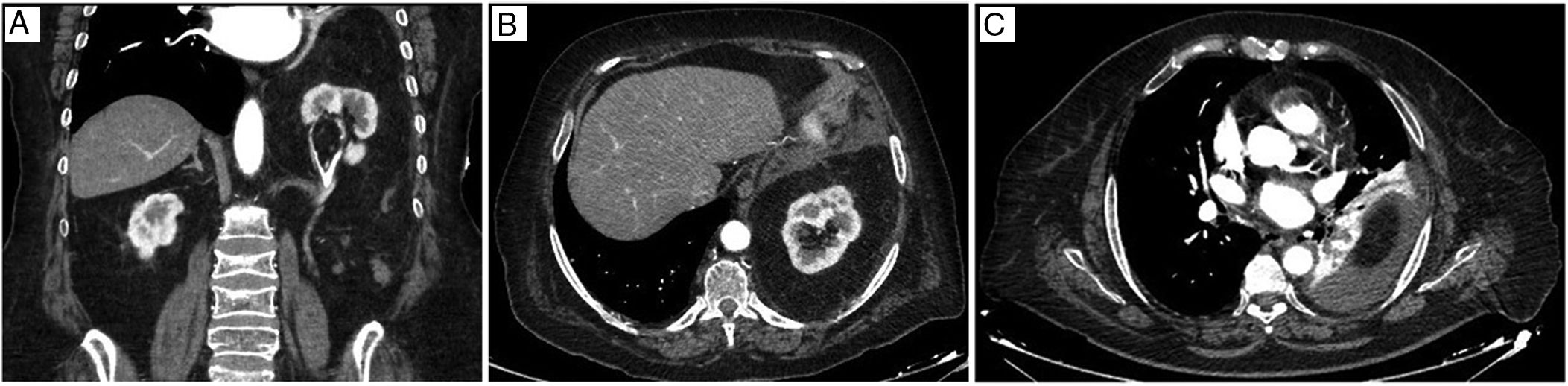
We report the case of an 80-year-old woman with a history of cholecystectomy who consulted for pain in the right iliac fossa. Examination revealed signs of peritonitis in the mesogastrium, and blood tests showed raised levels of acute phase reactants. Computed tomography was performed, showing segmental bowel wall thickening in the context of probable ileitis, a Bochdalek diaphragmatic hernia (BDH) containing the left kidney (Fig. 1A), and pleural effusion with underlying atelectasis of the left lower lobe (Fig. 1B and C).
The absence of respiratory disease and renal involvement led us to take a wait-and-see approach with regard to the BDH. The patient was admitted for medical treatment of ileitis, with satisfactory progress.
The incidence of BDH is 1/4000–5000 neonates, and it occurs more often in women. In most cases, the pleuroperitoneal fusion defect is posterolateral and left-sided, and contains small intestine (90%), omentum, stomach, colon, spleen, and exceptionally the kidney.1 The neonatal form causes respiratory failure due to pulmonary hypoplasia, and requires stabilization, tracheal and nasogastric intubation, and urgent intervention. Only 5% are diagnosed in adulthood, when they tend to be asymptomatic. Surgery is proposed in case of obvious symptomatology or risk of complications. Reduction of the hernia contents, sac resection and closure of the orifice, with or without prosthetic material, is recommended, usually by laparoscopy from an abdominal approach.2
Please cite this article as: Perfecto Valero A, Serrano Hermosilla C, Fernández Fernández J. Hernia de Bochdalek con contenido de riñón izquierdo intratorácico. Arch Bronconeumol. 2019;55:587.







