


We present a case of a 54-year-old man with a four-month shortness of breath history; his chest radiograph showed patchy partially linear peripheral lower zone predominant opacities, and a prominent right hilum (Fig. 1A). A chest computer tomography (CT) scan (Fig. 1B–E) revealed extensive serpiginous interlobular septal thickening around the secondary pulmonary lobules in the lower lobes, without pleural thickening or effusion. Notably, there was a consolidation in the right upper lobe with prominent right hilar lymph nodes. CT-guided biopsy and fluorodeoxyglucose positron emission tomography (FDG PET) CT (Fig. 1F, G) were negative for malignancy. To rule out sarcoidosis, a video-assisted thoracoscopy (VATS) for a right lung diagnostic wedge resection and paratracheal lymph node sampling was performed. Histopathology was compatible with congenital pulmonary lymphangiectasia; the lymph node showed lymphatic dilatation. On subsequent CT following a pulmonary embolism suspicion, the septal thickening had progressed (Fig. 1H).
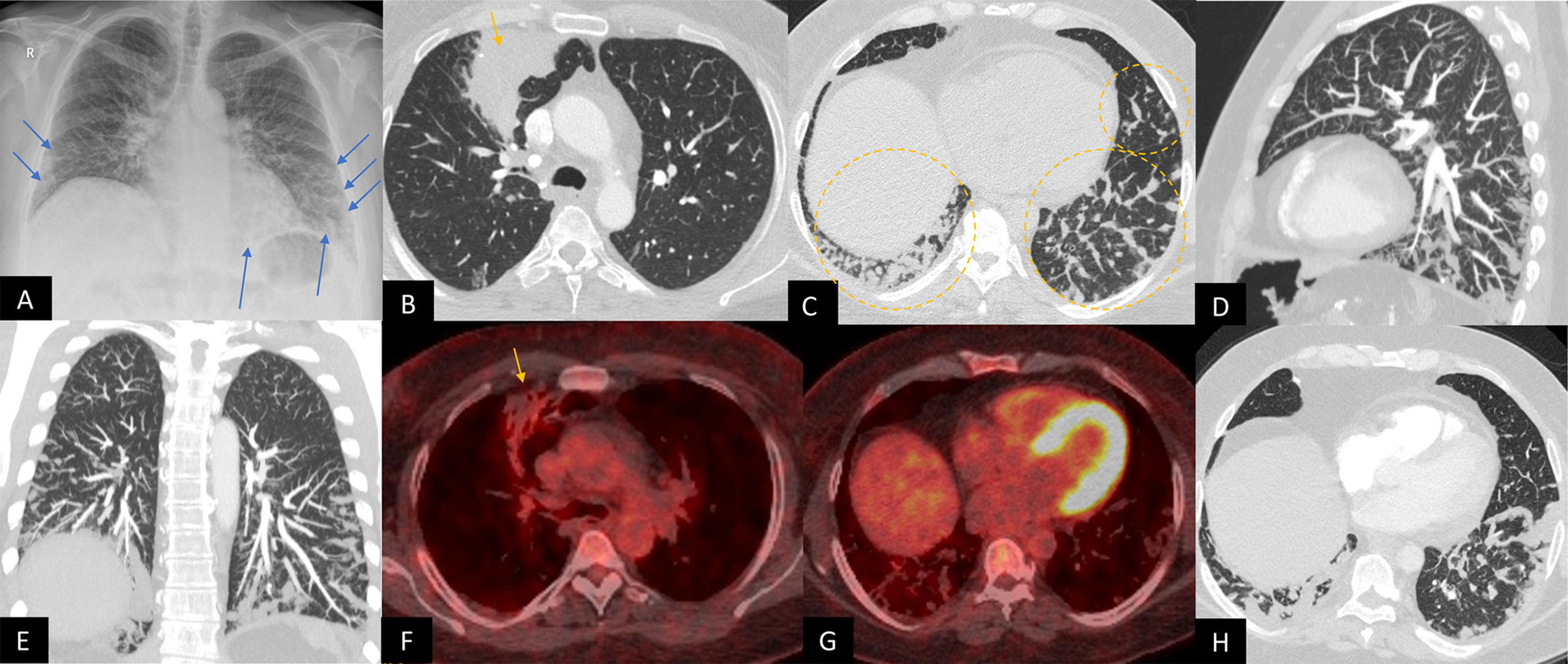
 Posteroanterior chest radiograph in erect position, showing patchy partially linear peripheral opacities in the lower zones (blue arrows). Allowing for incomplete inspiratory effort and elevated right hemidiaphragm, the right hilum also appears prominent. (B) CT chest study, axial plane in lung window showing a consolidation in the right upper lobe (yellow arrow) with prominent right hilar lymph nodes. (C) CT chest study, axial plane in lung window showing extensive smooth interlobular serpiginous septal thickening (yellow dashed circles) representing prominent dilated nodular lymphatic channels around the secondary pulmonary lobules in the lower lobes. Note there is no pleural effusion; there was no pleural thickening. (D, E) CT chest study, minimum intensity projection (10mm) in sagittal and coronal views, respectively, highlighting the shape and distribution of lower zone predominant serpiginous septal thickening. (F, G) Fused FDG PET-CT images in axial view show a resolving right upper lobe consolidation of low avidity (yellow arrow), as well as non-avid septal thickening in the lower zones. (H) CT pulmonary angiogram acquired 4 years later for a suspicion of pulmonary embolism, axial view, lung window shows progression of the septal thickening, with maintained shape patterns. There was no pulmonary embolism.")
(A) Posteroanterior chest radiograph in erect position, showing patchy partially linear peripheral opacities in the lower zones (blue arrows). Allowing for incomplete inspiratory effort and elevated right hemidiaphragm, the right hilum also appears prominent. (B) CT chest study, axial plane in lung window showing a consolidation in the right upper lobe (yellow arrow) with prominent right hilar lymph nodes. (C) CT chest study, axial plane in lung window showing extensive smooth interlobular serpiginous septal thickening (yellow dashed circles) representing prominent dilated nodular lymphatic channels around the secondary pulmonary lobules in the lower lobes. Note there is no pleural effusion; there was no pleural thickening. (D, E) CT chest study, minimum intensity projection (10mm) in sagittal and coronal views, respectively, highlighting the shape and distribution of lower zone predominant serpiginous septal thickening. (F, G) Fused FDG PET-CT images in axial view show a resolving right upper lobe consolidation of low avidity (yellow arrow), as well as non-avid septal thickening in the lower zones. (H) CT pulmonary angiogram acquired 4 years later for a suspicion of pulmonary embolism, axial view, lung window shows progression of the septal thickening, with maintained shape patterns. There was no pulmonary embolism.
While adult congenital pulmonary lymphangiectasia is rare, the distribution pattern and shape suggest a pulmonary lymphatic dilatation.1,2 The differentials include interstitial lung edema, sarcoidosis, and lymphangitis carcinomatosa. Thick septa in serpiginous shapes in lower zone distribution without associated lymphadenopathy, nodules and pleural disease help to narrow the differential. CT and MRI lymphangiography may aid in determining the aetiology in unclear cases.2
FundingNo funding was received for this work.
Conflict of interestsAuthors have no competing interests to declare.







