


We report a case of a 64-year-old man diagnosed with pulmonary thromboembolism 10 months ago with radiological progression despite anticoagulant treatment. The patient presents dyspnea and chest pain. 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET-CT) showed a hypermetabolic intraluminal solid lesion in the left main pulmonary artery (Suv 8.3) with heterogeneous contrast enhancement and extension to the interlobar artery and upper lobe artery (Fig. 1). Echobronchoscopy showed the occupation of the pulmonary artery by an isoechogenic material with anechoic irregular areas. Elastography shows a predominantly rigid lesion. We performed an Endobronchial ultrasound-guided transbronchial fine needle aspiration (EBUS-TBNA) with a 21G needle and EBUS guided mediastinal cryobiopsy (EBUS-MCB) with a 1.1mm cryoprobe (Fig. 2). There weren’t relevant complications, just a little bleeding. The pathological result was intimal sarcoma of the pulmonary artery (Fig. 3). The patient was treated with left pneumonectomy and resection of the sarcoma on the left pulmonary artery.
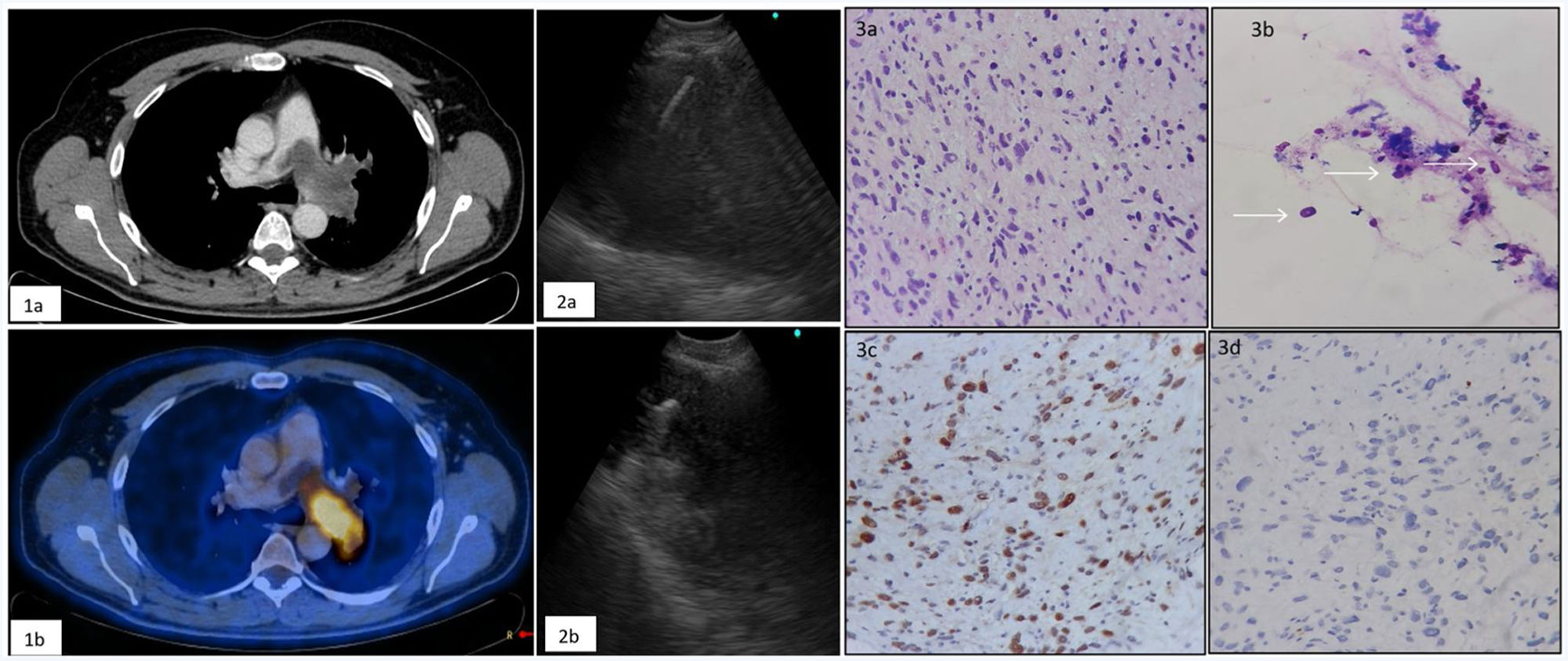
 Contrast-enhanced CT reveals a mild enhanced mass in the left pulmonary artery. (1b) 18F-fluorodeoxyglucose (FDG) positron emission tomography with integrated CT shows a positive uptake of FDG to the pulmonary artery mass. (2) Ultrasound image of fine needle (2a) and cryoprobe (2b) in the middle of the mass. (3) Hemtoxylin–eosin: atypical spindle cells with irregular, pleomorphic, large spindle-shaped nuclei, with elongated cytoplasms (3a,3b). Immunocytochemical study: MDM2++ positive tumor cells (3c) and negative for actine (3d).")
(1a) Contrast-enhanced CT reveals a mild enhanced mass in the left pulmonary artery. (1b) 18F-fluorodeoxyglucose (FDG) positron emission tomography with integrated CT shows a positive uptake of FDG to the pulmonary artery mass. (2) Ultrasound image of fine needle (2a) and cryoprobe (2b) in the middle of the mass. (3) Hemtoxylin–eosin: atypical spindle cells with irregular, pleomorphic, large spindle-shaped nuclei, with elongated cytoplasms (3a,3b). Immunocytochemical study: MDM2++ positive tumor cells (3c) and negative for actine (3d).
Pulmonary artery sarcoma (PAS) is a rare entity with an estimated global incidence of 0.001–0.03%.1 Histopathology reveals mesenchymal origin. More than half of the patients are misdiagnosed as pulmonary thromboembolism because symptoms (predominantly dyspnea, cough, and chest pain) and radiological images in chest angiotomography are very similar.1 PAS should be suspected in patients with chronic pulmonary thromboembolism with right heart failure due to pulmonary hypertension that doesn’t improve despite anticoagulant treatment. In these cases, PET-CT can differentiate the two entities based on the maximal standardized uptake value (SUVmax) that is significantly higher in pulmonary artery sarcoma. The diagnosis is histopathological.2 Surgical resection is considered the best option for treatment and adjuvant chemotherapy and radiation therapy may extend survival in some cases.3
The literature describes different alternatives to achieve sample for histopathological diagnosis: mediastinoscopy, EBUS-TBNA and Endovascular catheter Biopsy.1,3 In our case, we described the first case diagnosed using EBUS-MCB. This is a novel, minimally invasive technique with few complications.
EBUS allows better visualization of the tumor and vascular flow via Doppler ultrasonography but cytology obtained by TBNA shows limited percentage of viable tumor components. For that reason, MCB is a complementary procedure that allows to obtain large mediastinal samples with preserved tissue architecture for a better comprehensive morphophysiological and molecular diagnosis.1,2 The technique consists of applying cold with the cryoprobe (3–4s).
EBUS-MCB did not generate any relevant complications. Most frequent is light bleeding resulting from the previous puncture with the aspiration needle used in EBUS-TBNA. Other less frequent complications such as pneumothorax, mediastinitis, pneumomediastinum, and hemomediastinum, have been described in a small percentage of cases.4,5
If we compare EBUS-MCB with the methods used for the diagnosis of PAS, it is a cost-effective, fast, and minimally invasive technique, with few complications. Moreover, we obtain a larger sample than with EBUS-TBNA, which avoids the need for re-biopsies. Therefore, if pulmonary artery sarcoma is suspected in a location accessible to the EBUS, it could be considered as a diagnostic option.
Conflict of interestsThe authors state that they have no conflict of interests.







