


Neonatal pneumonia (NP) is one of the most common diseases causing dyspnea and hospitalization in neonates. In the last ten years, lung ultrasound (LUS) has been successfully used in the diagnosis and differential diagnosis of various neonatal lung diseases, including NP.1–3 Due to the high sensitivity and specificity of LUS in the diagnosis of pneumonia, the clinical application of LUS is increasing.2–4
Recently, several scholars have attempted to distinguish the etiology of pneumonia, especially to distinguish between bacterial and viral pneumonia, according to the size of the lung consolidation area on ultrasound. Berce et al. suggested that a diameter>2.1cm is a diagnostic factor for bacterial pneumonia with a sensitivity of 80% and a specificity of 75%, while for viral pneumonia, the extent of consolidation is small, with a size<2.0cm.5 Similarly, other studies have shown that bacterial, viral, or atypical pneumonia can be distinguished based on the extent of lung consolidation on ultrasound images.6–8
However, according to our more than 12 years of research on LUS and pneumonia and our experience in clinical practice, we believe that the above opinions or conclusions are not correct and that their scientific basis and reliability are questionable. This paper further investigates this issue based on typical cases or the literature and from the following aspects to aid in the correct development and better application of LUSs and to avoid misleading readers.
- 1.
LUS can aid in the accurate diagnosis of neonatal pneumonia
LUS can accurately diagnose pneumonia, including neonatal,1,9 pediatric10–12 and adult pneumonia.13,14 According to the international expert consensus, the diagnosis of pneumonia by LUS relies mainly on the following manifestations.15 (1) Lung consolidations are accompanied by air bronchograms with irregular or jagged boundaries. Consolidations may be located at one or more positions in the lung field, and consolidated areas may differ in size and shape in different lung fields. (2) The pleural line is abnormal, and the A-lines have disappeared. (3) B-lines or alveolar-interstitial syndrome (AIS) are visible in the nonconsolidated areas. (4) Different degrees of unilateral or bilateral pleural effusion are visible in some infants. (5) The main manifestations of mild or early pneumonia may present as small subpleural focal consolidations and AIS.
- 2.
Pneumonia caused by different pathogens can have the same or similar ultrasound manifestations
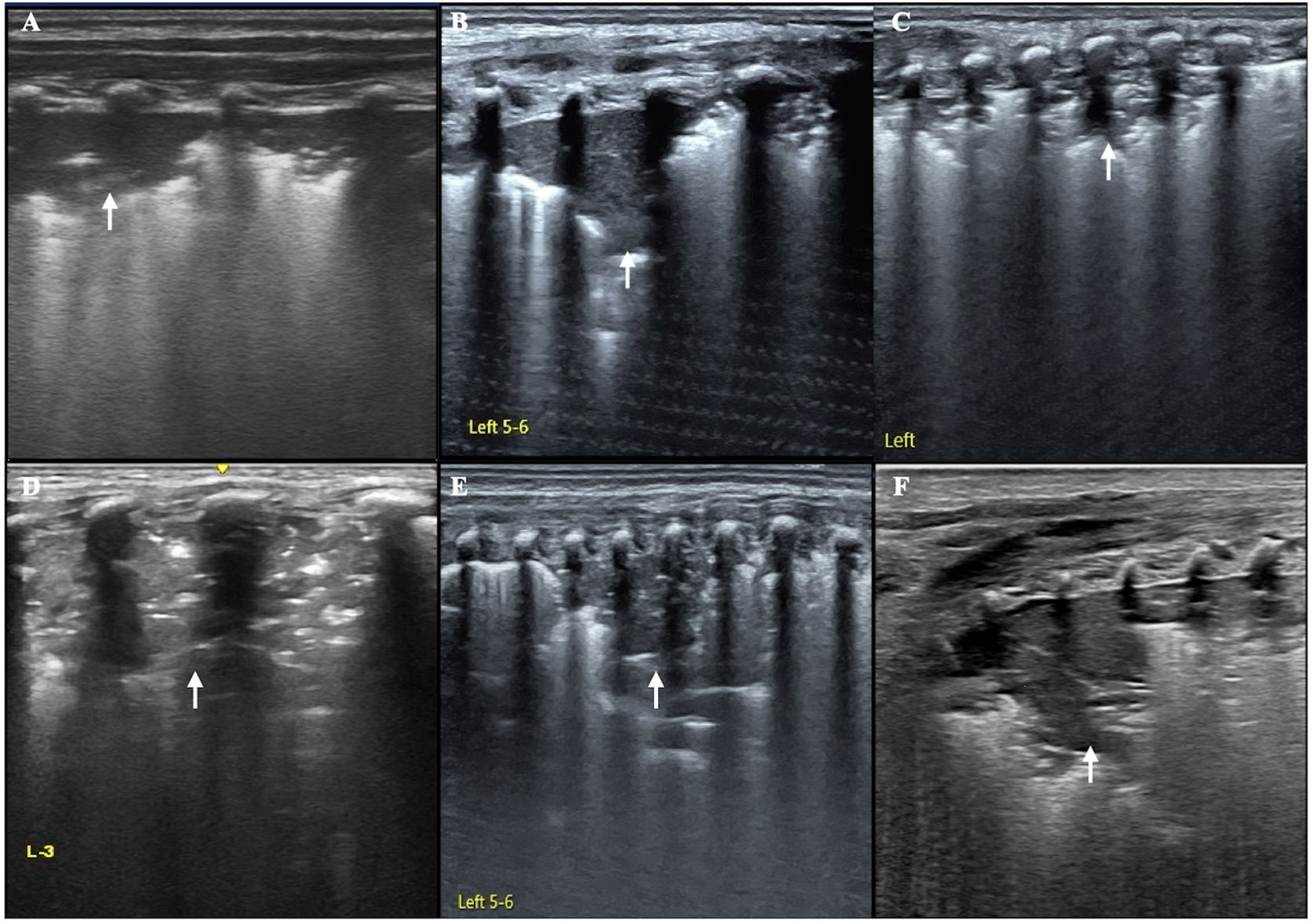
Recently, our group conducted a prospective, multicenter, 10-hospital study involving 135 patients with pathogen-identified neonatal infectious pneumonia. The results showed that pneumonia caused by different pathogens (such as bacteria, fungi, viruses, and mycoplasma) has the same or similar ultrasound manifestations, and the main manifestation is lung consolidation with air bronchograms.9 Other studies have shown that there are no specific sonographic findings for fungal, bacterial, or viral pneumonia.1,3,16,17Fig. 1 illustrates the lack of correlation between the extent of consolidation by LUS and the specific etiological diagnosis of each pneumonia (Fig. 1).
 (A: Mycoplasma pneumoniae). B: Candida albicans-related pneumonia. C: Respiratory syncytial virus pneumonia. D: Klebsiella pneumoniae pneumonia. E: Legionella pneumonia. F: E. coli pneumonia).") Fig. 1.
Fig. 1.Ultrasound findings of different types of pneumonia caused by different pathogens. This figure shows that pneumonia caused by various pathogens that mainly manifests as lung consolidation with air bronchograms and irregular boundaries on ultrasound images (arrow) (A: Mycoplasma pneumoniae). B: Candida albicans-related pneumonia. C: Respiratory syncytial virus pneumonia. D: Klebsiella pneumoniae pneumonia. E: Legionella pneumonia. F: E. coli pneumonia).
(0.27MB). - 3.
Congenital pneumonia, nosocomial pneumonia and community-acquired pneumonia can all have the same or similar ultrasound manifestations
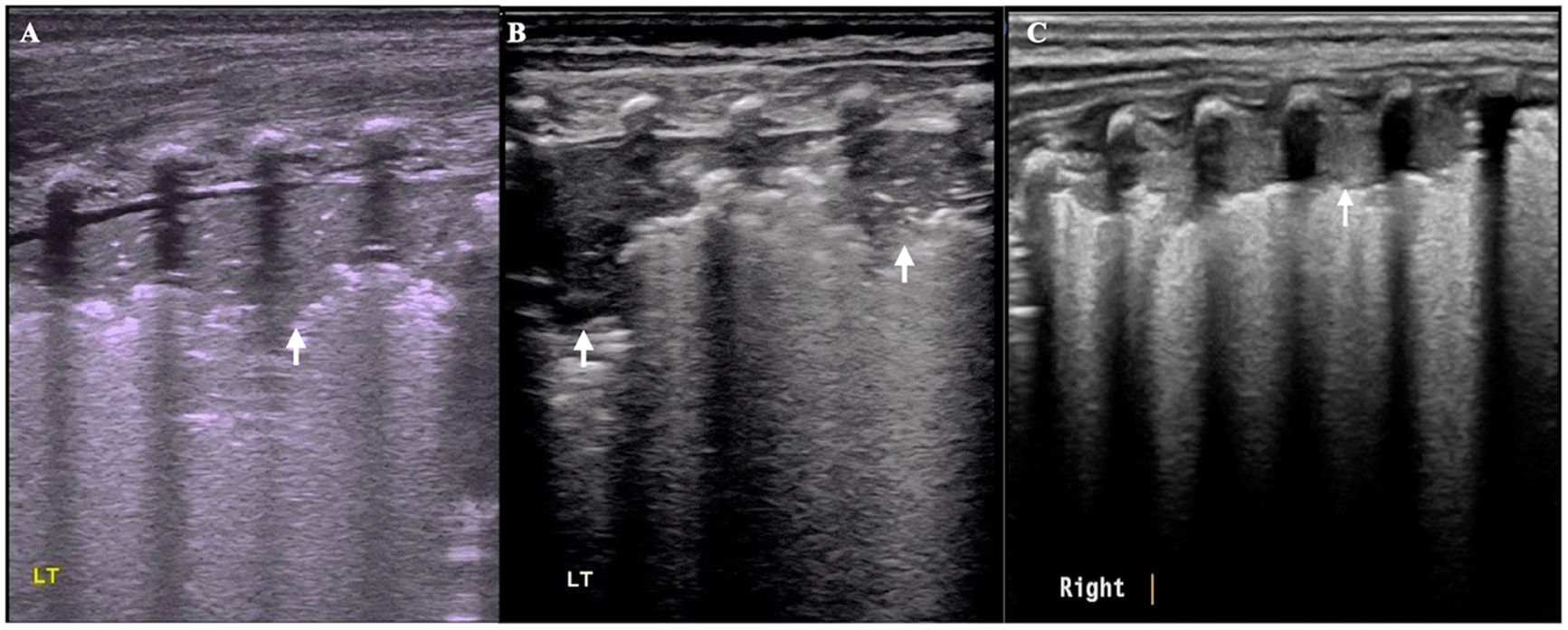
According to the time of onset, neonatal infectious pneumonia can be divided into congenital (that is, intrauterine infection) pneumonia, nosocomial infection (including ventilator-associated pneumonia) and community-acquired pneumonia. Studies have shown that these types of pneumonia also exhibit similar sonographic imaging patterns, that is, varying degrees of lung consolidation with air bronchograms as well as irregular or jagged boundaries.2,3,10,16,17Fig. 2 also shows that identifying the pathogen according to the manifestations of LUS is difficult in patients with congenital, nosocomial or community-acquired pneumonia (Fig. 2).
, nosocomial pneumonia (B) and community-acquired pneumonia (C) were similar. The main manifestations were significant lung consolidation involving multiple intercostal spaces with or without air bronchograms and regular boundaries (arrow).") Fig. 2.
Fig. 2.Comparison of the ultrasound features among patients with congenital pneumonia, nosocomial pneumonia and community-acquired pneumonia. As shown in this figure, the ultrasound manifestations of congenital pneumonia (A), nosocomial pneumonia (B) and community-acquired pneumonia (C) were similar. The main manifestations were significant lung consolidation involving multiple intercostal spaces with or without air bronchograms and regular boundaries (arrow).
(0.17MB). - 4.
Pneumonias with different properties (infectious or aspiration) can have the same or similar ultrasound manifestations.
According to the different classification methods used, neonatal pneumonia can also be divided into infectious pneumonia and aspiration pneumonia, among which aspiration pneumonia can be further divided into milk aspiration pneumonia and meconium aspiration pneumonia. According to our long-term study and clinical application of lung ultrasound, aspiration pneumonia and infectious pneumonia are also very consistent in terms of their appearance on ultrasound imaging.9,18,19
- 5.
Different age groups of patients with pneumonia can have the same or similar ultrasound manifestations
According to our studies and the literatures, the main sonographic manifestations of pneumonia in newborns, children and adults are similar or the same, which are all different degrees of lung consolidation with air bronchogram. Therefore, it is impossible to distinguish among different age groups based on ultrasound findings.1,9–15
In conclusion, the extent of lung consolidation is not related to the infecting pathogen, but to the severity of the lung disease.9 Severe inflammation in the lungs induced by bacteria or viruses can lead to substantial lung consolidation.20 Conversely, if the disease is mild, the extent of consolidation can be minimal, even in patients with bacterial pneumonia.9 Therefore, we can determine the severity of pneumonia based on the extent of lung consolidation but cannot discriminate the causative agent and the nature of the pneumonia. Microbiological diagnosis of pneumonia still depends on pathogen detection technology. In addition, it should be noted that the above studies on the discrimination of viral or bacterial pneumonia with LUS did not describe whether the images were acquired with vertical or parallel scans when LUS was performed. Vertical scans can display the lung consolidation involving multiple intercostal spaces simultaneously, while parallel scans can only display area involving one intercostal space. With the increasing application of LUS in the management of severe patients in every medical field, standardized operation is particularly important.
 (A: Mycoplasma pneumoniae). B: Candida albicans-related pneumonia. C: Respiratory syncytial virus pneumonia. D: Klebsiella pneumoniae pneumonia. E: Legionella pneumonia. F: E. coli pneumonia).")
, nosocomial pneumonia (B) and community-acquired pneumonia (C) were similar. The main manifestations were significant lung consolidation involving multiple intercostal spaces with or without air bronchograms and regular boundaries (arrow).")
Dr. Jing Liu contributed all of the aspects to this work, including conceptualizing and designing the study, data collection and analysis, drafting, reviewing and critically revising the manuscript, as well as approved the final manuscript as submitted.
Ethics approval and consent to participateThere is no needed to this work.
FundingThere was no funding or support available for this study.
Conflict of interestsNo conflict of interest.







