

Although asthma is one of the most prevalent chronic respiratory diseases, the participation of Spanish pulmonology units in the management of asthma may have room for improvement.
ObjectiveTo determine the degree of involvement of the Spanish pulmonology services in the patient care, education and research related with asthma disease and especially in difficult-to-control asthma.
MethodsA survey made up of 75 questions was sent to the heads of several pulmonology departments. The survey asked questions pertaining to respiratory disease care in general, and in asthma in particular, as well as the educational activities and research in asthma during the previous five years.
ResultsOut of the 107 surveys sent, 69 (645%) centers filled them out and returned them. Forty-seven (681%) met the criteria for an important level of health-care activity in asthma. However, only 29 (42%) had a monographic consultation for difficult-to-control asthma and 37 (536%) used an education program. As for postgraduate education, only 31 (449%) provided their resident physicians with specific asthma training. And in the research field, 12 (174%) reported having projects funded by SEPAR and 25 (362%) had published studies in journals with an impact factor.
ConclusionsAlthough the majority of the pulmonology centers interviewed report a notable activity in asthma patient care, their involvement in the specialized approach for difficult-to-control asthma is insufficient. Likewise, participation in educational activities and research related with the disease is inconsistent and limited to few centers.
Si bien el asma es una de las enfermedades respiratorias crónicas más prevalentes, existe la sospecha de que la participación de los centros de neumología españoles en su manejo es potencialmente mejorable.
ObjetivoDeterminar el grado de implicación de los servicios de neumología españoles en la asistencia, docencia e investigación relacionadas con la enfermedad asmática y específicamente con la de control difícil.
MétodoSe remitió una encuesta formada por 75 ítems que cumplimentaron los responsables de los centros entrevistados. La encuesta interrogaba sobre la asistencia neumológica general y la del asma en particular, así como la actividad docente e investigadora en la enfermedad asmática en los cinco años previos.
ResultadosDe las 107 encuestas enviadas, 69 (64,5%) centros las retornaron cumplimentadas. De estos, 47 (68,1%) reunieron criterios de actividad asistencial destacada en asma. Sin embargo, solo 29 (42%) disponían de una consulta monográfica de asma de control difícil y 37 (53,6%) utilizaban un programa de educación. En el ámbito docente, únicamente 31 (44,9%) proporcionaban formación específica sobre asma a sus médicos residentes. Y en el de investigación, 12 (17,4%) referían tener proyectos subvencionados por SEPAR y 25 (36,2%) habían publicado trabajos en revistas con factor de impacto.
ConclusionesSi bien la mayoría de los centros neumológicos entrevistados refieren una notable actividad en la asistencia del asma, su implicación en el abordaje especializado del asma de control difícil es insuficiente. Así mismo, su participación en actividades docentes y de investigación relacionadas con la enfermedad es desigual y limitada a escasos centros.
Asthma is one of the most prevalent chronic respiratory diseases. Recent studies confirm that the morbidity and mortality of the disease are substantially decreasing in developed countries.1,2 This improvement is probably related with the therapeutic advances made in recent years, and fundamentally with the generalized use of inhaled glucocorticosteroids as a preventive treatment.3,4 However, other studies consistently show that in 30%–55% of asthma patients, the disease is insufficiently controlled.5,6 Therefore, due to its high prevalence and poor control, asthma is still a priority disease in pulmonology. The Spanish Society of Pulmonology and Thoracic Surgery (SEPAR) and its Asthma Group, and more recently with the Integrated Research Program (PII), lead the involvement of Spanish medical services in the disease. Several health-care, educational and research initiatives show evidence of this leadership.7–10
Nevertheless, the considerable development recently experienced in several more technological areas of modern pulmonology (sleep apnea-hypopnea syndrome, non-invasive ventilation, etc.) could have favored a proportional decline in the interest of specialists in asthma. This circumstance, together with the lower morbidity and mortality in asthma, may condition the current training of resident pulmonologists in asthma. As this training takes place in hospital centers, the reduced frequency of asthma cases treated in hospitals may have led to residents having fewer opportunities to treat patients with asthma. Nowadays, the disease is more often treated in the ambulatory setting rather than in hospitals, and current resident physician training programs in teaching hospitals dedicate a limited time to said activity. This contrasts with regulations of the current training program for resident physicians specializing in pulmonology in Spain (BOE, Orden SCO 2605/2008), according to which pulmonologists in training must acquire theoretical and practical knowledge in order for them to competently deal with asthma patient care.
Therefore, it is essential to determine the current involvement of pulmonology units and departments in asthma patient care, education and research in our country. If an optimal level is not met, this verification could lead to the establishment of corrective measures in the future. Currently, there is either no information available about this situation or, at best, it is fragmentary and insufficient.
Under these premises, from the Area of Asthma and in collaboration with the Continuous Medical Training Committee (Comité de Formación Médica Continuada – FMC) of SEPAR, the ATENEA Program was designed, whose main objective was to complete the standard training in asthma of resident physicians in pulmonology by means of short stays at Spanish hospitals that are recognized for their high level of involvement in the disease. With the intention of impartially identifying said centers, a survey was developed and sent to Spanish pulmonology departments and units, which was done similarly as in previous experiences in other areas of knowledge in this specialty.11 Therefore, the survey's aim was to determine the degree of involvement declared by the Spanish pulmonology centers themselves in the overall management of asthma, and particularly in difficult-to-control asthma.
Methods and MaterialsStudy DesignA cross-sectional study designed to determine the involvement in asthma patient care, post-graduate education and research of the 107 Spanish pulmonology departments and units registered in the SEPAR database. The information was collected with a survey that had been developed for this purpose and was sent by both postal mail and e-mail in February and May 2008 to the heads of the workgroups.
SurveyThe survey was made up of 75 items asking about: (a) general health-care activities and resources of the pulmonology department or unit: type of hospital, number of beds, area of influence and population, type of unit dedicated to chest disease activities, technical and human resources; (b) specific asthma-related health-care activity and resources: treatment of exacerbations, number of visits in the outpatient consultation, specific difficult-to-control asthma consultation, specific human and technical resources; and (c) teaching and research activity specific to asthma during the previous 5 years: organization of post-graduate courses, availability of a specific asthma educational program for resident physicians, university professors in the unit, research interns or biologists, participation in projects promoted by the Health-Care Research Fund (Fondo de Investigación Sanitaria – FIS) or SEPAR, participation in CIBER (Spanish acronym for Centers for Basic Research in Respiratory Diseases) or RTIC (Integrated Thematic Network of Centers) research networks or groups, participation in and number of clinical assays, number of original publications with impact factor and number of doctoral theses completed.
A center was considered to have “outstanding health-care activity in asthma” if it had at least one of the following characteristics: an asthma unit; a consultation specializing in difficult-to-control asthma; and a pulmonologist, nurse or allergist preferentially dedicated to the specialized care of asthma patients.
Statistical AnalysisA descriptive analysis of the sample was completed for all the variables compiled. The values are expressed as percentages and frequencies. We compared the equipment and the activities of the centers identified as having “outstanding health-care activity in asthma” with the rest of the centers without “outstanding health-care activity in asthma”. The means of the two groups were compared with the Student's t-test for the quantitative variables and the χ2-test for the qualitative variables. When it was considered opportune, the results were expressed as odds ratio (OR) with their 95% confidence interval (CI). In order to identify the variables that were independently associated with the circumstance of having a consultation specialized in difficult-to-control asthma, a multivariate logistic regression analysis was performed. The model included the independent variables of the study that showed significant differences in the univariate analysis. In all cases, the level of statistical significance was established at 5% (α=0.05). The data analysis was done with the SPSS program (version 18.0) for Windows (SPSS, Inc., Chicago, IL, USA).
ResultsOut of the 107 surveys that had been sent, 69 were correctly completed and returned (64.5%), all of which are included in the final analysis. Table 1 shows the geographical distribution of the participating pulmonology departments and units. Out of these, 39 (56.5%) were pulmonology departments located at hospitals with more than 500 beds, 21 (30.5%) were pulmonology departments or sections in centers with 250–500 beds and 9 (13%) were functional units in centers with less than 250 beds. The general health-care activities and the equipment of the participating pulmonology centers are compiled in Table 2. More than 94% stated having available a hospital ward, outpatient consultation, complete lung function facilities, bronchoscopy and a respiratory sleep disorder unit.
Geographical Location of the 69 Centers That Completed the Survey.
| Alicante | 1 |
| Asturias | 3 |
| Badajoz | 1 |
| Baleares | 3 |
| Barcelona | 12 |
| Burgos | 1 |
| Cáceres | 1 |
| Cádiz | 1 |
| Cantabria | 1 |
| Ceuta | 1 |
| Córdoba | 1 |
| Coruña | 1 |
| Girona | 2 |
| Granada | 2 |
| Guadalajara | 2 |
| Huelva | 1 |
| Huesca | 1 |
| Las Palmas | 2 |
| León | 1 |
| Lleida | 2 |
| Lugo | 1 |
| Madrid | 10 |
| Málaga | 2 |
| Murcia | 2 |
| Navarra | 1 |
| Orense | 1 |
| Sevilla | 2 |
| Valencia | 6 |
| Vizcaya | 2 |
| Zaragoza | 2 |
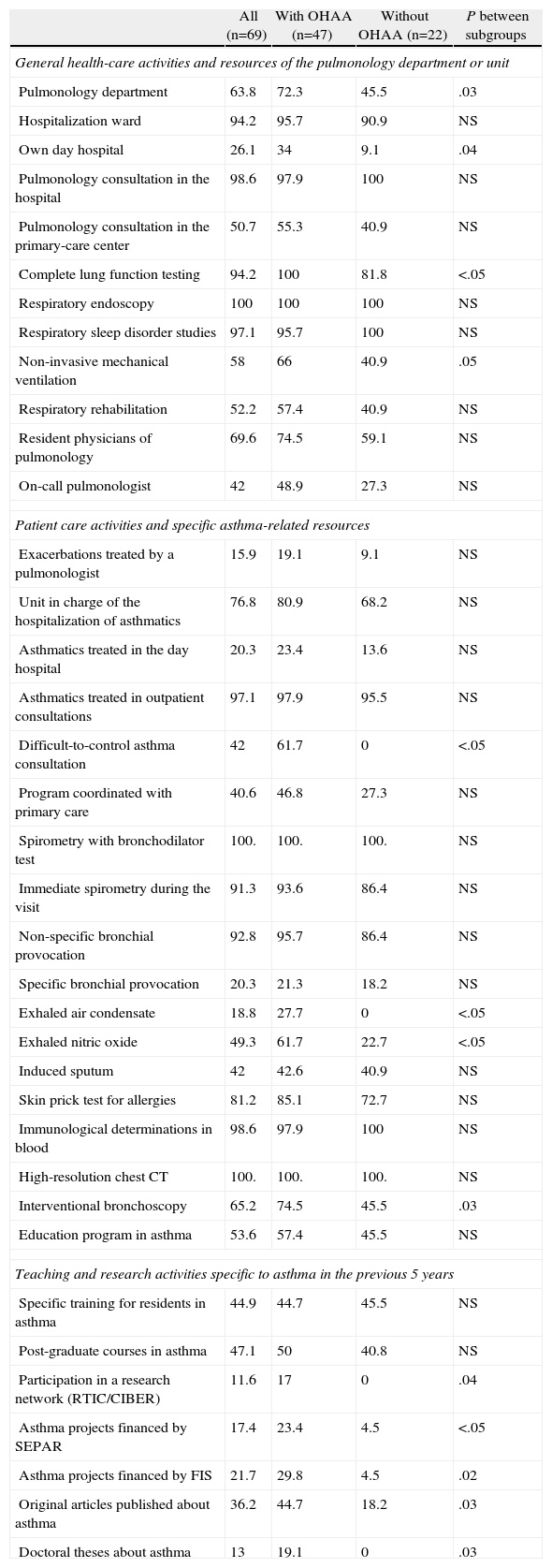
Characteristics of the Care Provided and General Pulmonology Resources As Well As Those Specific to Asthma of All the Centers Surveyed, Distributed According to Whether or Not They Met the Criteria for “Outstanding Health-Care Activity in Asthma” (OHAA).
| All (n=69) | With OHAA (n=47) | Without OHAA (n=22) | P between subgroups | |
| General health-care activities and resources of the pulmonology department or unit | ||||
| Pulmonology department | 63.8 | 72.3 | 45.5 | .03 |
| Hospitalization ward | 94.2 | 95.7 | 90.9 | NS |
| Own day hospital | 26.1 | 34 | 9.1 | .04 |
| Pulmonology consultation in the hospital | 98.6 | 97.9 | 100 | NS |
| Pulmonology consultation in the primary-care center | 50.7 | 55.3 | 40.9 | NS |
| Complete lung function testing | 94.2 | 100 | 81.8 | <.05 |
| Respiratory endoscopy | 100 | 100 | 100 | NS |
| Respiratory sleep disorder studies | 97.1 | 95.7 | 100 | NS |
| Non-invasive mechanical ventilation | 58 | 66 | 40.9 | .05 |
| Respiratory rehabilitation | 52.2 | 57.4 | 40.9 | NS |
| Resident physicians of pulmonology | 69.6 | 74.5 | 59.1 | NS |
| On-call pulmonologist | 42 | 48.9 | 27.3 | NS |
| Patient care activities and specific asthma-related resources | ||||
| Exacerbations treated by a pulmonologist | 15.9 | 19.1 | 9.1 | NS |
| Unit in charge of the hospitalization of asthmatics | 76.8 | 80.9 | 68.2 | NS |
| Asthmatics treated in the day hospital | 20.3 | 23.4 | 13.6 | NS |
| Asthmatics treated in outpatient consultations | 97.1 | 97.9 | 95.5 | NS |
| Difficult-to-control asthma consultation | 42 | 61.7 | 0 | <.05 |
| Program coordinated with primary care | 40.6 | 46.8 | 27.3 | NS |
| Spirometry with bronchodilator test | 100. | 100. | 100. | NS |
| Immediate spirometry during the visit | 91.3 | 93.6 | 86.4 | NS |
| Non-specific bronchial provocation | 92.8 | 95.7 | 86.4 | NS |
| Specific bronchial provocation | 20.3 | 21.3 | 18.2 | NS |
| Exhaled air condensate | 18.8 | 27.7 | 0 | <.05 |
| Exhaled nitric oxide | 49.3 | 61.7 | 22.7 | <.05 |
| Induced sputum | 42 | 42.6 | 40.9 | NS |
| Skin prick test for allergies | 81.2 | 85.1 | 72.7 | NS |
| Immunological determinations in blood | 98.6 | 97.9 | 100 | NS |
| High-resolution chest CT | 100. | 100. | 100. | NS |
| Interventional bronchoscopy | 65.2 | 74.5 | 45.5 | .03 |
| Education program in asthma | 53.6 | 57.4 | 45.5 | NS |
| Teaching and research activities specific to asthma in the previous 5 years | ||||
| Specific training for residents in asthma | 44.9 | 44.7 | 45.5 | NS |
| Post-graduate courses in asthma | 47.1 | 50 | 40.8 | NS |
| Participation in a research network (RTIC/CIBER) | 11.6 | 17 | 0 | .04 |
| Asthma projects financed by SEPAR | 17.4 | 23.4 | 4.5 | <.05 |
| Asthma projects financed by FIS | 21.7 | 29.8 | 4.5 | .02 |
| Original articles published about asthma | 36.2 | 44.7 | 18.2 | .03 |
| Doctoral theses about asthma | 13 | 19.1 | 0 | .03 |
Values in percentages of the group.
CT: computed tomography; FIS: Spanish acronym for Health-Care Research Fund; RTIC/CIBER: Spanish acronyms for Integrated Thematic Network of Centers/Centers for Basic Research in Respiratory Diseases; SEPAR: Spanish acronym for Spanish Society of Pulmonology and Thoracic Surgery.
Information related with the health-care activity and the specific equipment for asthma is shown, as we have mentioned, in Table 2. Among the other results observed, we have seen that the majority of the centers were equipped for basic techniques (spirometry, non-specific bronchial provocation, allergy skin prick testing) to provide basic health-care services for asthma patients. The mean number of patients treated annually for asthma in the outpatient consultations (information not shown in Table 2) was 787 (minimum of 50, maximum 3340). Only 29 (42%) workgroups had a specialized difficult-to-control asthma consultation and 37 (53.6%) offered an asthma education program.
The main variables used for analyzing the post-graduate training and research activities specific for asthma in the five previous years are also shown in Table 2. Within the realm of post-grad work, it is striking that only 31 (44.9%) of the centers surveyed provided their resident physicians with specific asthma training; when contemplated as a whole, these centers employed a total of 116 university professors and had offered 171 post-grad courses in asthma. As for research activities, only 12 (17.4%) and 15 (21.7%) of the departments carried out any type of research in asthma funded by government agencies (like FIS) or scientific societies (SEPAR), respectively, and 25 (36.2%) had published one or more original articles about asthma in biomedical journals with an impact factor. The total breakdown of resources and research activities included: 13 biologists and 8 research interns; 16 doctoral theses; participation in 37 FIS and 24 SEPAR projects; 143 original articles published in biomedical journals with an impact factor; and 209 clinical assays completed (information not shown in Table 2).
In accordance with the pre-established parameters, 47 (68.1%) centers met the criteria for “outstanding health-care activity in asthma”. As observed in Table 2, these departments and units, when compared with those without “outstanding health-care activity in asthma”, were shown to be significantly better equipped (day hospital, non-invasive mechanical ventilation, complete lung function testing, interventionist bronchoscopy, determination of exhaled nitric oxide and exhaled condensate) and to have specialized difficult-to-control asthma consultations (61.7% vs 0%). There were no statistically significant differences between the centers of both groups for the number of physicians or resident physicians assigned to the department or unit. There were also no significant differences in the mean number of patients treated annually for asthma in the hospital outpatient consultations: 823 (762) vs 695 (800), respectively. However, the centers with “outstanding health-care activity in asthma” presented a significantly greater scientific activity with a greater participation in research networks (RTIC/CIBER) and a higher number of original publications in journals with an impact factor (2.96 [4.2] vs 0.2 [0.3], P=.01) and doctoral theses (0.3 [0.8] vs 0 [0], P=.05).
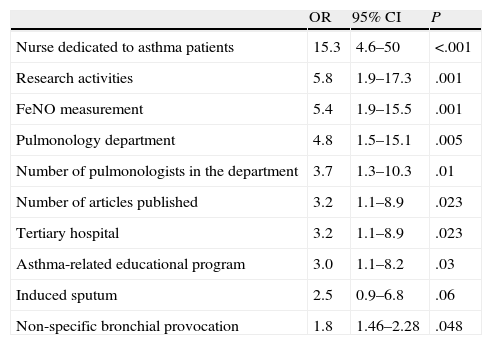
Table 3 demonstrates the variables that were associated with having a specialized difficult-to-control asthma consultation. No differences were observed between the centers either with or without a difficult-to-control asthma consultation for the following variables: availability of spirometry on the day of the consultation (96.6/87.5%); skin prick testing for allergies (82.8/80%); blood immunology analysis (100/98.6%); participation in clinical assays (79.3/60%); having resident physicians (79.3/62.5%); specific training in asthma for resident physicians (48.3/42.5%); and preparation of doctoral theses (20.7/7.5%). The multivariate analysis revealed that the variables that were associated with having a specific difficult-to-control asthma consultation were: having a nurse specifically dedicated to dealing with asthma patients (OR: 13.3; 95% CI: 3.8–46) and being involved in asthma research (OR: 4.5; 95% CI: 1.2–16.9).
Variables in the Univariate Analysis Associated With Having a Specialized Consultation for Difficult-to-Control Asthma in the Center. Values Expressed as Odds Ratio (OR) and 95% Confidence Interval (CI).
| OR | 95% CI | P | |
| Nurse dedicated to asthma patients | 15.3 | 4.6–50 | <.001 |
| Research activities | 5.8 | 1.9–17.3 | .001 |
| FeNO measurement | 5.4 | 1.9–15.5 | .001 |
| Pulmonology department | 4.8 | 1.5–15.1 | .005 |
| Number of pulmonologists in the department | 3.7 | 1.3–10.3 | .01 |
| Number of articles published | 3.2 | 1.1–8.9 | .023 |
| Tertiary hospital | 3.2 | 1.1–8.9 | .023 |
| Asthma-related educational program | 3.0 | 1.1–8.2 | .03 |
| Induced sputum | 2.5 | 0.9–6.8 | .06 |
| Non-specific bronchial provocation | 1.8 | 1.46–2.28 | .048 |
FeNO: fraction exhaled nitric oxide.
One of the main contributions of this present study is that the results of the survey describe the current situation in Spain of asthma-related health-care services, education and research in pulmonology departments and units. This information, which goes beyond the simple description of the situation, could serve as a basis for designing future improvements in those areas that are susceptible to intervention. In overall terms, the results lead towards notable activity in the management of the disease, as was supposed, but with less participation in specialized care for difficult-to-control asthma and in post-graduate education and research specific to asthma, which was limited to a minority of the centers.
Generally, the pulmonology departments and units that were consulted reported being satisfactorily technically equipped for the basic care of patients with respiratory pathologies. More than 94% of the centers had a hospital floor or ward available for hospitalizations, an outpatient consultation, complete lung function study facilities, bronchoscopy and a respiratory sleep disorder unit. As for asthma patient care, the centers surveyed reported a relevant volume of asthma patients seen in their outpatient consultations (787patients/year) and more than 80% had the basic techniques necessary to do so, such as spirometry with bronchodilator test, non-specific bronchial provocation, skin prick test for allergies and immunological determinations in blood. On the other hand, it should be noted that a high proportion of the participating centers admitted not having a specific education program for the treatment of the disease (46.4%) or a specialized difficult-to-control asthma consultation (58%). Both observations merit specific comments.
Difficult-to-control asthma is probably the variation of the disease in which the expertise of the pulmonologist is most necessary. Although it affects a minority of patients out of the total asthma patient population (less than 4%),12 it results in important social and economic costs. Some studies estimate that the treatment of difficult-to-control asthma represents more than 50% of the total expenditure of the overall treatment of the disease.13,14 A proper diagnostic and therapeutic approach entails highly specialized care. Current immunomodulatory or biological therapies (omalizumab) and future ones (mepolizumab),15 used specifically in asthma treatment, require proper clinical evaluation. Even in the future, the foreseeable administration of mepolizumab will entail a rigorous classification of the bronchial inflammation (phenotype) and of the eventual candidates for this therapy, which will probably require the use of special complementary tests (eosinophil count in induced sputum). In addition, given the high cost of said treatments and from a standpoint of efficacy, in the future the public health-care system will probably require that its indication would meet rigorous criteria of efficacy based on data originating in test-based medicine. And consequently, it will demand a very specialized evaluation of the indication of the drug and of the follow-up of these patients. Therefore, given the high economic impact (due to its morbidity and special treatment) and the complex clinical care of difficult-to-control asthma, it has been recommended that the patients affected by this particular form of the disease should be seen in specialized units or consultations that are able to offer a highly qualified overall vision of the patient and his/her disease.16,17 The observation of the present study, where only 42% of the self-evaluated centers had a specialized difficult-to-control asthma consultation, is that the reality of the situation does not meet the mentioned recommendation. Nevertheless, similar studies done in other geographical areas confirmed even worse results. Roberts et al.,18 in a similar survey of pulmonologists in the United Kingdom, revealed that only 22.7% of the subjects interviewed had in their hospital a unit or consultation for difficult-to-control asthma. On the other hand, other results of our study reveal the logical association between having a difficult-to-control asthma consultation with showing preferential dedication to the disease (having a specialized nurse and doing research). Although these data could help identify some of the variables to consider for promoting its creation, we cannot obviate the probable selection bias in the inclusion of the variables considered in the multivariate analysis, in such a way that the reverse may be true. This would mean that the existence of a difficult-to-control asthma unit implies (or precedes) the participation of specialized nurses and asthma-related research activities.
The current clinical practice guidelines for asthma, both international19 and national,9 catalogue the efficacy of educational programs in asthma with the highest possible level of evidence (A). Consequently, they recommend their use in all patients, constituting an essential part of the treatment of the disease. This affirmation contrasts with the low proportion of centers with educational programs for asthma that we have seen in this study. On the other hand, this finding agrees with other observations made in our setting. One study that interviewed more than 1000 doctors and nurses familiarized with the follow-up of asthma patients revealed that only 16% of those interviewed stated that in their health-care centers there was a structured and individualized education program.20 This situation uncovers an aspect that requires specific actions to be taken.
The main result observed in the evaluation of the centers surveyed about their participation in educational activities in asthma is the low proportion (44.9%) of the application of a training program specifically directed at resident physicians of pulmonology. This observation seems to translate the perception of those in charge of teaching at the centers that asthma does not require specific, programmed training, unlike what happens with other areas within the specialty. For example, in order to acquire the necessary knowledge and skills related with bronchoscopy, respiratory sleep diseases or lung function, the resident physicians follow specific training programs. It is quite possible that the asthma training of said physicians is currently limited to merely treating asthma patients who have been hospitalized due to a severe exacerbation of the disease during the residents’ rotation on the hospital ward. This is undoubtedly insufficient, especially given the progressive decline in the number of patients with severe asthma exacerbation who require hospitalization,1 patients who on the other hand represent a trifling percentage of the asthmatic population. Today, asthma is a preeminently ambulatory disease. It is difficult for physicians in training to acquire the essential knowledge and understanding of the disease in order to make diagnoses, establish the level of control and particularly to manage drug prescriptions and dosages (which temporarily change according to the level of control) of asthma maintenance treatment if they have not received a minimum of training in such matters. In conclusion, the limited time that is usually assigned to training in ambulatory pulmonology (due to the 4-year training period limitation) and the general lack of asthma-specific programs observed are probably providing pulmonology resident physician with insufficient preparation. The need for a greater dedication to education in asthma could be an additional argument in favor of those who see the need to increase the training period for resident physicians of pulmonology to five years instead of the current four.
The research activity evaluated as a whole (143 publications, 37 FIS projects, 24 SEPAR projects, 16 doctoral theses, 209 clinical assays) is an appreciable scientific production. However, said production was not universal and was limited to 12 (17.4%) centers that stated having projects funded by SEPAR and 25 (36.2%) articles published in biomedical journals with an impact factor over the last 5 years. This observation demonstrates that the scientific interest in the disease is limited to a select group of centers. The uneven participation observed in the research setting of asthma coincides with the lack of growth seen years ago compared with other more dynamic areas of pulmonology, for instance respiratory sleep disorders, which has experienced considerable growth over the same time period.21,22
The comparison between the centers distributed as to whether or not they reported “outstanding health-care activity in asthma” provided some interesting observations. Although there were differences between both groups regarding some of the complementary techniques available (measurement of exhaled nitric oxide and exhaled condensate, bronchoscopy), others of greater relevance—such as human resources (number of physicians on staff or resident physicians in the department), patient load (annual visits for asthma in the outpatient consultations), the basic explorations used in asthma care (spirometry, non-specific bronchial provocation, skin prick tests for allergies) and their participation in post-graduate education—were similar. Despite this, the centers with an “outstanding health-care activity in asthma” reached significantly better indices in the research parameters evaluated (funded research projects, original publications, doctoral theses); therefore, it could be interpreted that this observed greater productivity would be more closely associated with the personal interest of the members of said centers and their involvement in asthma than with the center's facilities or patient load.
The study design, based on a self-administered survey, could have some potential limitations. On one hand, some of the questions asked about specific numerical data, such as the number of office visits or publications, and documents backing these answers were not requested. Although the answers given were held to be true, there may be a certain degree of bias of the interviewee towards exaggerating these values. Nevertheless, in our opinion, said observation does not call into question the scope of the conclusions, particularly of the more negative ones, such as the partial implication of certain centers in educational and research activities. In any event, it would reflect a better scenario of the actual reality, which would not change the negativity of the results. On the other hand, from the initial list of participating units, only 64.5% answered the survey. Nevertheless, said proportion of answers can be considered satisfactory compared with other studies with similar characteristics. In the study by Roberts et al. only 50.4% responded. In our study, given that 56.5% of the answers came from the departments of tertiary hospitals, we consider that the results at least describe the situation in the better-equipped centers that are leaders in excellent pulmonology health-care, including in asthma, in Spain.
In short, the health care provided for asthma patients in Spanish pulmonology departments and units, in terms of general care and resources used, seems appropriate. However, specialized care for difficult-to-control asthma as well as quality post-graduate education and research in this disease is partial and restricted to certain centers. These results identify areas for future improvement and give meaning to recent SEPAR initiatives (by the Asthma Area and Asthma PII) in order to increase training in the specialized care of the disease of resident physicians of pulmonology (ATENEA Program) and incentives for asthma research for young pulmonologists (Grupo Emergente de Asma, SEPAR).
FundingThis study has been sponsored by the Asthma Area of SEPAR (Spanish acronym for Spanish Society of Pulmonology and Thoracic Surgery). Unconditional aid was also received by AstraZeneca, which did not intervene in the data collection, analysis, interpretation of the results or drafting of the manuscript.
Conflict of InterestsThe authors declare having no conflicts of interest related to this study.
We would like to thank the participating centers who filled out the survey voluntarily, to the technical administration of SEPAR for the information given by the centers and AstraZeneca for sponsoring the ATENEA Program.
Please cite this article as: Plaza V, et al. Implicación de los servicios de neumología españoles en la asistencia, docencia e investigación en asma. Resultados de la encuesta ATENEA. Arch Bronconeumol. 2012;48:114–119.







