


Residential radon is the second most important risk factor for lung cancer and the first among never-smokers. The objective of this study is to report the concentrations of residential radon in a series of never-smoker cases recruited in a multicenter study of cases and controls in northwestern Spain. In this study, all the hospitals in the Spanish province of Galicia and one from Asturias participated.
Patients and methodsThe present article includes a series of cases with residential radon measurements. All the subjects were personally interviewed, 3ml of blood was taken from each, and they were each given instructions about how to place a residential radon detector in their homes.
ResultsSixty-nine case subjects were recruited, 84% of whom were women with a mean age of 71% and 81% of whom had adenocarcinoma. The average concentration of residential radon in the cases was 237Bq/m3, while the average concentration in the Galician population is 79Bq/m3. No relationship was observed between the concentration of residential radon and either sex or age at the time of diagnosis of the cases, but there was a tendency towards having a greater concentration in those diagnosed with small-cell and large-cell carcinoma.
ConclusionsThe concentrations of residential radon in the cases included are very high at about three times the average concentration of residential radon to which the general population of Galicia is exposed.
El radón residencial es el segundo factor de riesgo del cáncer de pulmón y el primero en nunca fumadores. El objetivo de este estudio es describir la concentración de radón residencial en una serie de casos nunca fumadores reclutados en un estudio multicéntrico de casos y controles en el noroeste de España. En este estudio participan todos los hospitales gallegos y uno asturiano.
Pacientes y métodosEn el presente artículo se incluye la serie de casos con mediciones de radón residencial. A todos los casos se les realiza una entrevista personal, se les extraen 3ml de sangre total y se les dan instrucciones para la colocación de un detector de radón residencial en su domicilio.
ResultadosSe han incluido 69 casos (el 84% mujeres), con una edad media de 71 años y el 81% con adenocarcinoma. La concentración mediana de radón residencial en los casos ha sido de 237Bq/m3, mientras que la concentración mediana en la población gallega es de 79Bq/m3. No se ha observado relación entre la concentración de radón residencial y el sexo o la edad al diagnóstico de los casos, pero sí hay una tendencia a tener mayor concentración en los diagnosticados de carcinoma de células pequeñas y de células grandes.
ConclusionesLas concentraciones de radón residencial en los casos incluidos son muy elevadas, del orden de 3 veces la concentración mediana de radón residencial a la que está expuesta la población general gallega.
Lung cancer is currently a serious health-care problem. According to data of the Spanish National Institute of Statistics, it was the cause of 20401 deaths in 2009, becoming the third cause of death in Spain after ischemic heart disease and cerebrovascular diseases. According to sex, there were 17279 deaths in men and 3122 in women; in order, lung cancer was the second and thirteenth cause of death, respectively.1 In addition to its high incidence, it is also highly lethal. According to recent data, 5-year survival after diagnosis ranges from 12% to 16%.2,3 This survival rate has hardly improved in recent decades and early diagnosis of the disease is therefore essential, as are the need to improve primary prevention activities by eliminating its main risk factors and improving treatments.
Lung cancer is a multifactorial disease.4 It is attributed to smoking in 79% of all cases in men and 47% in women.5 It has been reported that exposure to residential radon is the second cause of lung cancer in smokers and the first in never-smokers.6 More and more studies indicate that lung cancer in never-smokers is a different molecular entity than lung cancer in smokers,7–10 and the study of its risk factors is very useful in order to understand its etiology. However, few research studies have exclusively analyzed lung cancer in never-smokers and none, as far as we know, has been specifically aimed at finding out exactly what is the effect of residential radon exposure in these patients.
Radon is a colorless, odorless, insipid gas that appears during the disintegration chain of uranium 238. At semi-disintegration, radon emits radioactive alpha particles that, when they impact with the cells of the pulmonary epithelium, may cause genetic-molecular alterations and ultimately cause cancer. As alpha particles do not penetrate, they release all their energy in a micrometrical space. Radon has a half-life of 3.8 days; therefore its inhalation is barely a health risk. There are, however, descendants of radon that have a very short half-life (especially polonium 214) that represent a true risk for lung cancer. The radon that is exhaled from the Earth's crust tends to become concentrated in the inside of buildings and, therefore, the risk for lung cancer tends to increase in subjects who are exposed to higher concentrations. Galicia and certain areas of the Iberian Peninsula are risk areas due to the geological substrate on which they lie.11–13 For this reason, we consider it especially interesting to analyze the contribution of exposure to residential radon to lung cancer in never-smokers. Previous studies in Galicia have consistently observed that, even at concentrations within recommended levels,12 radon is an important risk factor for lung cancer that could participate in up to 25% of all lung cancer deaths. In Galicia, this could represent one death per day due to this disease.14
The results that are presented in this article are part of a more extensive study (LCRINS – Lung Cancer Risk in Never Smokers), a multicenter study with international projection. All the hospitals in Galicia and one hospital in Asturias participate in this study, whose objective is to identify risk factors for lung cancer in never-smokers and their possible interaction with certain genetic polymorphisms. The specific objective of this study is to report the residential radon concentrations in a series of cases of lung cancer in never-smokers and to correlate them with several characteristics of said cases (sex, age at diagnosis or histologic type).
Subjects and MethodsStudy Design and SettingThe LCRINS study has a hospital-based case–control design. The cases are subjects with confirmed anatomic pathology diagnosis of lung cancer who have smoked: (a) less than 100 cigarettes in their life; or (b) no more than one cigarette per day for 6 months.
The study is being carried out at the following hospitals: Complejo Hospitalario Universitario in A Coruña (CHUAC), Hospital Universitario Lucus Augusti (Lugo), Complejo Hospitalario Arquitecto Marcide (Ferrol), Complejo Hospitalario Universitario in Santiago de Compostela (CHUS), Complejo Hospitalario Universitario in Pontevedra (CHOPO), Complejo Hospitalario Universitario in Vigo (CHUVI), Policlínica in Vigo (POVISA), Complejo Hospitalario Universitario in Ourense (CHOU) and Hospital Central in Asturias.
The study has been funded by a competitive research project grant from the government of Galicia (10CSA208057PR), and its protocol and informed consent forms have been approved by the Ethics Committee for Clinical Research of Galicia (registration number 2010/295).
Patient Recruitment and Data CollectionThis present study reports only the results of the first few cases included in the LCRINS study and their residential radon exposure.
The researchers of each center performed a search of active cases. When a case was detected, the patient completed a survey that asks about different life-style aspects: exposure to second-hand smoke (in the home and during childhood), prior occupations, leisure activities that could entail greater lung cancer risk (DIY projects, painting, model-making),15,16 diet and alcohol consumption. In addition, the cases were given instructions for placing a residential radon detector along with the detector itself and a postage-paid envelope in order to send the detector to the center of the study coordinator three months after its placement. After giving informed consent, 3ml of blood was withdrawn from each participant. The questionnaires and total blood were sent by express mail to the coordinating center the same day of the interview. In order to guarantee proper placement of the detector and its return by mail, 2 phone calls were made to the participants: one after the detector was given to the participant by the researcher, and another when the period of residential radon measurement had concluded.
Measurement of Residential Radon ConcentrationsOnce the detectors were received together with a survey about characteristics of the house where they had been placed, the residential radon concentration was determined at the Galician Radon Laboratory, located at the Hospital Clínico Universitario in Santiago de Compostela. The measurement system used was by optical microscope and an automatic count of traces with the Radosys 2000® system. The measurement system involved a calculation algorithm that included seasonal adjustments and duration of the exposure period, among other factors. Periodical determinations were taken from non-exposed (blank) detectors as a quality control of the measurement instrument. The Galician Radon Laboratory has participated with excellent results in intercomparison exercises promoted by the Spanish Nuclear Security Council.17,18 Once the concentrations of residential radon were determined, the participants were sent letters with the results and recommended actions to take in cases where the maximum recommended concentration had been exceeded.
Statistical AnalysisA descriptive univariate analysis was done of the subjects included in the study. To report the concentration of residential radon, measurements were used that were based on ordinations instead of central tendency measurements due to the fact that the distribution is log-normal. A bivariate analysis was done to compare the possible differences in residential radon concentrations regarding age of diagnosis, sex of the cases and histologic type of lung cancer. In some cases, the result of the bivariate analysis is shown with block diagrams and comparisons are made using the non-parametric Mann–Whitney U-test, considering a P value <.05 significant. For the analysis, we used PASW Statistics, version 18.
ResultsParticipation in the StudyIn the present article, we have included all those cases whose residential radon concentrations had been measured up until May 2012. Although the LCRINS study includes 108 cases (as of 16/05/2012), we only have had the measurements of 69 of these cases up until the indicated date. The radon detector was initially placed in the homes of 79 cases, but for several reasons (death, loss of the detector, could not locate the participant), 10 participants did not return the detector, which represents a return rate of 87.3%.
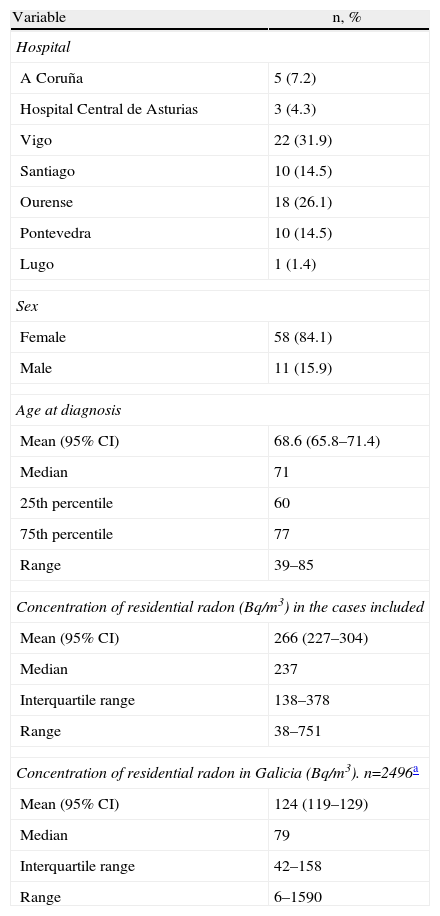
Characteristics of the Study SubjectsThe characteristics of the subjects included are shown in Table 1. Somewhat more than half of the participants came from the hospitals in Ourense and Vigo, and there is a clear predominance of women among the cases. Mean age at diagnosis was around 71 (interquartile age range 60–77), and 25% of the never-smokers were diagnosed at age 60 or younger. The predominant histologic type was adenocarcinoma, diagnosed in 81% of the cases. Mean concentration of residential radon in the homes of the included cases was 237Bq/m3.
Characteristics of the Never-smoker Cases With a Measurement of Residential Radon (n=69).
| Variable | n, % |
| Hospital | |
| A Coruña | 5 (7.2) |
| Hospital Central de Asturias | 3 (4.3) |
| Vigo | 22 (31.9) |
| Santiago | 10 (14.5) |
| Ourense | 18 (26.1) |
| Pontevedra | 10 (14.5) |
| Lugo | 1 (1.4) |
| Sex | |
| Female | 58 (84.1) |
| Male | 11 (15.9) |
| Age at diagnosis | |
| Mean (95% CI) | 68.6 (65.8–71.4) |
| Median | 71 |
| 25th percentile | 60 |
| 75th percentile | 77 |
| Range | 39–85 |
| Concentration of residential radon (Bq/m3) in the cases included | |
| Mean (95% CI) | 266 (227–304) |
| Median | 237 |
| Interquartile range | 138–378 |
| Range | 38–751 |
| Concentration of residential radon in Galicia (Bq/m3). n=2496a | |
| Mean (95% CI) | 124 (119–129) |
| Median | 79 |
| Interquartile range | 42–158 |
| Range | 6–1590 |
Regarding the age at diagnosis, those over the age of 70 presented a mean concentration of residential radon higher than that of younger subjects (300 vs 212Bq/m3; Mann–Whitney U P=.387). Fig. 1 demonstrated the difference in the radon concentrations between both diagnostic age groups. As for sex, there are no appreciable differences in the concentrations of residential radon between men and women. The median concentration of radon in the males’ homes was 199Bq/m3, vs 238Bq/m3 in the females’ homes (Mann–Whitney U, P=.412), although there are only 11 males out of the 69 participants. Fig. 2 shows the distribution of the radon concentrations for both sexes.


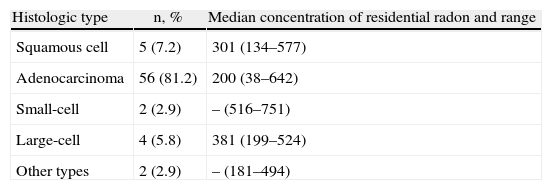
Regarding the concentration of residential radon and its relationship with the histologic type of lung cancer, it is observed that the lowest concentration correlates with adenocarcinoma, while the highest concentration is for large-cell and small-cell carcinoma, although there are only 4 and 2 cases, respectively, of these histologic types among the 69 patients included. The description of the histologic types and radon concentration for each can be seen in Table 2.
Concentration of Residential Radon and Histologic Type of Lung Cancer in Never-smokers (n=69).
| Histologic type | n, % | Median concentration of residential radon and range |
| Squamous cell | 5 (7.2) | 301 (134–577) |
| Adenocarcinoma | 56 (81.2) | 200 (38–642) |
| Small-cell | 2 (2.9) | – (516–751) |
| Large-cell | 4 (5.8) | 381 (199–524) |
| Other types | 2 (2.9) | – (181–494) |
This study shows that the concentrations of residential radon are high in a series of lung cancer cases in never-smokers. The median observed concentration is 237Bq/m3, while the level considered in need of action by American authorities is situated at 148Bq/m3 and the WHO has recently recommended that levels should not be higher than 100Bq/m3. It has also been observed that there is a tendency for higher concentrations in those cases with large-cell and small-cell histologic types.
The concentration of radon observed among the participants in the study is almost 3 times higher than the average concentration of residential radon observed in almost 2500 homes in Galicia.19 All these homes are part of the Galician Radon Map. Almost 70% of these measurements have been obtained by randomly selecting the participating subjects (and therefore their homes), and the preliminary results were published in 2007.13 The remaining 30% of the homes measured were obtained from direct contact with the general population and controls from 2 studies of cases and controls about radon and lung cancer done by our group.12,20
The studies available today have observed that the risk for lung cancer due to residential radon could be higher in never-smokers compared with smokers. These studies come from the addition of pooling studies from European and American case–control research, with the consequent heterogeneity in the data collection.21,22 In the European pooling study, there was an observed dosage–response relationship between lung cancer risk and the concentration of residential radon in never-smokers. Individuals exposed to more than 400Bq/m3 have 1.7 (95% CI: 1.2–2.3) times more risk for lung cancer compared with those who are exposed to less than 25Bq/m3. The number of subjects in the high exposure level was low.21 Nevertheless, the effect of residential radon in never-smokers has shown conflicting results. Sandler et al.23 observed a non-significant excess risk of 0.141 in never-smokers for every 100Bq/m3. However, this effect was higher than that observed in the total of the analyzed sample. In the American pooling study, the effect of the exposure to residential radon was the same for smokers and never-smokers,22 and the same was observed in the Iowa study.24 In another recently published environmental study among subjects participating in the Cancer Prevention Study II, no effect was found for the exposure to residential radon in never-smokers,25 while Wilcox et al. have observed that the effect of radon on lung cancer was higher in never-smokers than in smokers.26 Studies in miners have also obtained contradictory results.27,28
The results of this study show that never-smoker men and women with lung cancer are exposed to similar concentrations of residential radon. We have not found studies that enable us to compare these results. Initially, there do not seem to be reasons to think of a differential effect, contrary to tobacco. Both risk factors may have different carcinogenic mechanisms. As for age, the cases diagnosed at a later age have higher radon concentrations, although the difference is not significant. One possible explanation would be that radon needs a longer induction period and that, therefore, older subjects have been exposed for longer periods. We also have not found studies that have compared age at diagnosis in never-smoker lung cancer patients.
As for the histologic type, the results agree with other research and previous studies done by our group. The evidence available consistently indicates that radon, as it is a risk factor for lung cancer in all histologic types, should have greater influence in small-cell cancer and in other histologic types (including large-cell carcinoma). The American pooling study had the highest risk for small-cell carcinoma, followed by other histologic types,22 like the European pooling and other studies.26 The same pattern has been observed for studies done in miners.28 This same pattern has recently been observed in a case–control study in Galicia.20
Northwestern Spain, and especially the province of Galicia, provides a unique opportunity to analyze the effect of residential radon exposure in never-smokers. Due to the high concentrations of residential radon produced by the geological characteristics of the subsoil, the conditions for “natural experimentation” enable us to clearly determine the dose–response effect of radon on lung cancer in never-smokers given the high variability in the concentrations. This fact is accentuated by the constructive characteristics of many single-family homes made of granite that contribute to the increased concentrations of interior radon.13 Another study that was carried out in an area of less geological risk for residential radon concentrations did not find an association between radon and lung cancer,29 which reinforces the importance of the characteristics of the subsoil in lung cancer risk attributable to radon gas in the home.
This research presents a series of limitations, including the presentation of the results of the concentrations of residential radon between lung cancer cases without having available the concentrations from controls. In coming months, these results will be made available. We believe, however, that these preliminary data sufficiently illuminate the importance of radon in the etiology of lung cancer in never-smokers. Another limitation is the sample size, although the 69 cases included in the present analysis are a relatively high number when one considers the infrequency of lung cancer in never-smokers. Lastly, other variables may influence in the appearance of lung cancer, such as occupation or exposure to second-hand smoke. Nevertheless, its relative importance in the appearance of lung cancer is much less when compared with the effect of radon.
On the other hand, this present study presents several advantages. Perhaps the most important of these is its multicenter nature, given the low incidence of lung cancer in never-smokers. This fact increases the external validity of the results and achieves a sample size that is sufficiently high enough to obtain precise conclusions about lung cancer risk factors in never-smokers. Another advantage is the ample variability of residential radon concentrations, linked with the fact that the study was done in a risk area, which makes it easier to find out the effect of residential radon in never-smokers. Furthermore, the number of unreturned detectors was very small, with a return rate of more than 85% as a result of the participating researcher's efforts and their follow-up phone calls to the patients. The unreturned detectors have been associated with participants with some type of comprehension problem or those who were in the final phases of life at the time of diagnosis.
The concentrations of residential radon in the cases included are very high, at around 3 times the average residential radon concentration to which the Galician general public is exposed.19 It is therefore necessary to make both the population and the administrations aware of the importance that this gas can have in the development of lung cancer, both in smokers as well as never-smokers, and to promote preventive measures that have been demonstrated to be effective at reducing home exposure to radon.
FundingThis study has been financed with a competitive research project grant from the Galician Provincial Government (Xunta de Galicia, ref. 10CSA208057PR).
Conflict of InterestsThe authors declare having no conflict of interests.
Please cite this article as: Ruano-Ravina A, et al. Exposición a radón residencial y cáncer de pulmón en nunca fumadores. Resultados preliminares del estudio LCRINS. Arch Bronconeumol. 2012;48:405–9.







