


According to recent data obtained from the RE-TAI study, 48.5% of patients with chronic obstructive pulmonary disease (COPD) in Spain have poor therapeutic adherence1 (determined by the Test of Adherence to Inhalers [TAI]).2 When the TAI data were combined with information from pharmacy refill rate (PRR) electronic records, the percentage of patients with poor adherence increased to almost 55%.1
Factors influencing therapeutic adherence are heterogeneous and include, but are not limited to, patient education, inhaler ease-of-use, and the complexity of the therapeutic regimen.3,4 Lack of adherence is, in turn, associated with poor disease control and reduced quality of life, and an increase in the use of resources and costs.3 Consequently, acting on factors such as health education that improve the therapeutic adherence of COPD patients can contribute substantially to an improvement in the disease. It is estimated that reductions in morbidity and mortality among respiratory patients who followed an education program were due primarily to their increased therapeutic adherence. No studies have been conducted to evaluate differences in therapeutic adherence in patients from sites which provide varying educational support. The aim of this study was to determine whether COPD patients treated in sites with greater involvement in education have better therapeutic adherence.
The RE-TAI project was an observational, cross-sectional study that included 410 COPD patients from 21 sites (11 respiratory medicine, 5 internal medicine, and 5 primary care). Demographic characteristics were collected and the TAI was completed in a single visit. Subsequently, principal investigators at the participating sites completed the Education Involvement Scale (EIE), an ad hoc questionnaire composed of 8 questions scored between 1 (never) and 5 (always). The relationship between the EIE score and the percentage of patients with intermediate or good adherence (TAI 10 ≥ 46) was analyzed with a univariate analysis. A multivariate analysis was performed to determine which variables (demographic and clinical) were independently associated with high adherence.
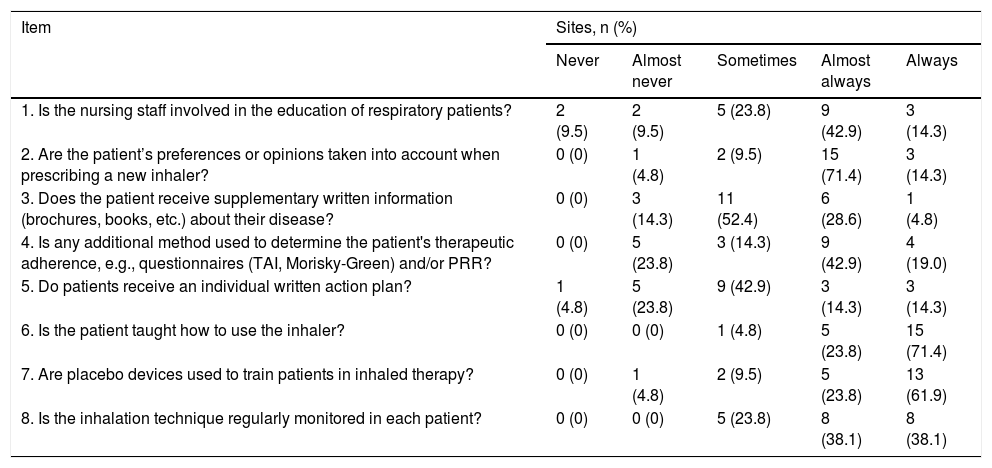
EIE scores per site ranged from 25 to 38, with a median (Q1-Q3) of 32 points (26–33) and a mean (SD) of 30.5 (4.1). More than 75% of sites reported that they always or almost always take patient preferences into account when prescribing the inhaler, instruct patients in its use using placebo inhalers, and monitor inhalation techniques (Table 1). Almost 62% of sites reported always or almost always using questionnaires or PRR to determine therapeutic adherence.
Responses from participating centers to the Educational Involvement (EIE) scale.
| Item | Sites, n (%) | ||||
|---|---|---|---|---|---|
| Never | Almost never | Sometimes | Almost always | Always | |
| 1. Is the nursing staff involved in the education of respiratory patients? | 2 (9.5) | 2 (9.5) | 5 (23.8) | 9 (42.9) | 3 (14.3) |
| 2. Are the patient’s preferences or opinions taken into account when prescribing a new inhaler? | 0 (0) | 1 (4.8) | 2 (9.5) | 15 (71.4) | 3 (14.3) |
| 3. Does the patient receive supplementary written information (brochures, books, etc.) about their disease? | 0 (0) | 3 (14.3) | 11 (52.4) | 6 (28.6) | 1 (4.8) |
| 4. Is any additional method used to determine the patient's therapeutic adherence, e.g., questionnaires (TAI, Morisky-Green) and/or PRR? | 0 (0) | 5 (23.8) | 3 (14.3) | 9 (42.9) | 4 (19.0) |
| 5. Do patients receive an individual written action plan? | 1 (4.8) | 5 (23.8) | 9 (42.9) | 3 (14.3) | 3 (14.3) |
| 6. Is the patient taught how to use the inhaler? | 0 (0) | 0 (0) | 1 (4.8) | 5 (23.8) | 15 (71.4) |
| 7. Are placebo devices used to train patients in inhaled therapy? | 0 (0) | 1 (4.8) | 2 (9.5) | 5 (23.8) | 13 (61.9) |
| 8. Is the inhalation technique regularly monitored in each patient? | 0 (0) | 0 (0) | 5 (23.8) | 8 (38.1) | 8 (38.1) |
PRR, Prescription refill record; TAI, Test of adhesion to inhalers.
Univariate analysis showed that intermediate or good adherence was significantly associated with the EIE score (OR: 1.09; 95% CI: 1.03–1.15; p = 0.002), while multivariate analysis showed that intermediate or good adherence was associated with a higher EIE score (OR: 1.08; 95% CI: 1.02–1.15; p = 0.011) and also with the number of inhalers used by the patient (OR: 1.53; 95% CI: 1.06–2.22; p = 0.024).
This study confirms that the degree of involvement of sites in their patients’ education may affect adherence to inhaled treatment in COPD patients. Other studies also suggest that certain strategies for patient empowerment, health education, and monitoring compliance increase adherence to inhaled treatment in these patients.5–9 Clinical practice guidelines also emphasize the importance of health education.10,11 These measures contrast with some observations from our study: e.g., no personalized action plans or written information, the involvement of nursing staff, or evaluation of therapeutic adherence using specific questionnaires or PRR. The heavy burden of care, the characteristics of COPD patients (age, comorbidities, polypharmacy, etc.), or even the lack of data from specialists on the use of inhalers12 could explain why there is such room for improvement in our country. Despite all this, COPD patients show a higher rate of unwitting non-compliance than, for example, asthmatic patients.13 Therefore, educational measures such as written self-management plans or visual aids, training in inhaler use, or audiovisual materials may be good strategies for improving adherence.5
This study has some limitations. The EIE used to assess the degree of health education in participating sites has not been previously validated. Moreover, only the principal investigator in each participating site completed the EIE, thus avoiding interpersonal differences between the different investigators who were able to recruit patients. The EIE has not been previously validated. The small series did not allow for comparisons between specialties. We intend to carry out a new, prospective study in a larger series that will include unbiased sites. Objectives will also include comparison between specialties. However, these potential limitations do not undermine the results obtained to date.
The authors express their appreciation to Chiesi for their sponsorship and GOC Networking for the technical support provided throughout the process.
Please cite this article as: Plaza V, Fernández C, Curto E, Alonso-Ortiz MB, Orue MI, Vega JM, et al. Adhesión terapéutica de los pacientes con EPOC según los niveles de implicación en educación sanitaria de sus centros. Arch Bronconeumol. 2021;57:307–309.







