


According to World Health Organization (WHO) 2014 estimates, 3.3% of new and 20% of previously treated cases of tuberculosis are due to multidrug-resistant tuberculosis (MDR-TB) strains.1
Unfortunately, outcomes of MDR- and extensively drug-resistant (XDR)-TB cases (particularly those with a resistance pattern beyond XDR-TB) are poor: therapeutic success is as low as 20%, and the failure and death rate is as high as 49%.2
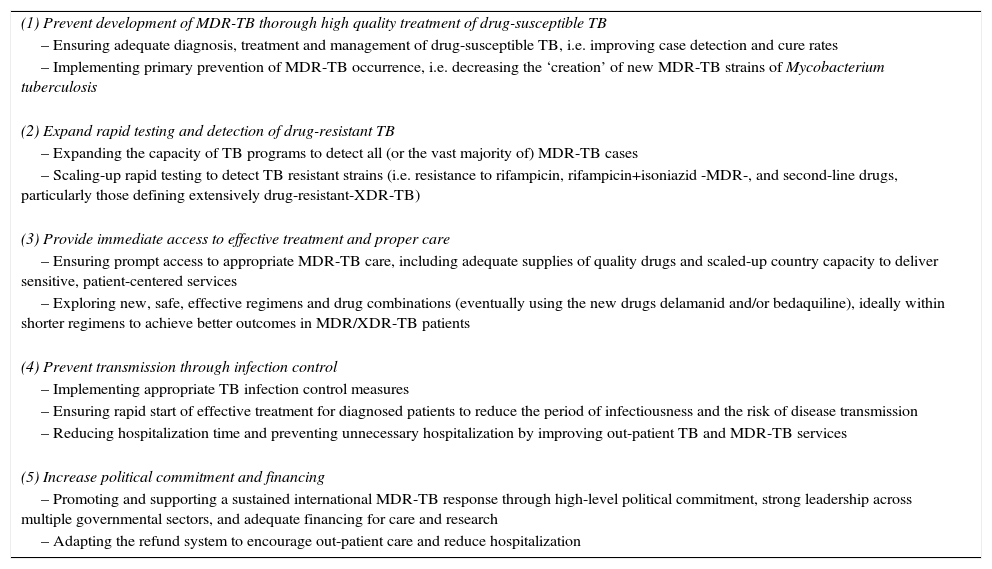
Recently, the WHO underlined the importance of proper management of MDR-TB,1,3–5 and outlined the priority actions to address the global MDR-TB crisis (Table 1).1
The 5 Priority Actions to Address the Global Multidrug-Resistant Tuberculosis (MDR-TB) Crisis.
| (1) Prevent development of MDR-TB thorough high quality treatment of drug-susceptible TB |
| – Ensuring adequate diagnosis, treatment and management of drug-susceptible TB, i.e. improving case detection and cure rates |
| – Implementing primary prevention of MDR-TB occurrence, i.e. decreasing the ‘creation’ of new MDR-TB strains of Mycobacterium tuberculosis |
| (2) Expand rapid testing and detection of drug-resistant TB |
| – Expanding the capacity of TB programs to detect all (or the vast majority of) MDR-TB cases |
| – Scaling-up rapid testing to detect TB resistant strains (i.e. resistance to rifampicin, rifampicin+isoniazid -MDR-, and second-line drugs, particularly those defining extensively drug-resistant-XDR-TB) |
| (3) Provide immediate access to effective treatment and proper care |
| – Ensuring prompt access to appropriate MDR-TB care, including adequate supplies of quality drugs and scaled-up country capacity to deliver sensitive, patient-centered services |
| – Exploring new, safe, effective regimens and drug combinations (eventually using the new drugs delamanid and/or bedaquiline), ideally within shorter regimens to achieve better outcomes in MDR/XDR-TB patients |
| (4) Prevent transmission through infection control |
| – Implementing appropriate TB infection control measures |
| – Ensuring rapid start of effective treatment for diagnosed patients to reduce the period of infectiousness and the risk of disease transmission |
| – Reducing hospitalization time and preventing unnecessary hospitalization by improving out-patient TB and MDR-TB services |
| (5) Increase political commitment and financing |
| – Promoting and supporting a sustained international MDR-TB response through high-level political commitment, strong leadership across multiple governmental sectors, and adequate financing for care and research |
| – Adapting the refund system to encourage out-patient care and reduce hospitalization |
We discuss here how the WHO priority actions can be used at the programmatic level to control MDR- and XDR-TB.
Prevent Development of MDR-TB Through High Quality Treatment of Drug Susceptible TBMathematical modeling suggests that best-practice short-course chemotherapy, by achieving cure rates over 80% in new cases, can control isoniazid- or rifampicin-resistant disease while preventing the emergence of MDR-TB,1 although existing drug-resistant cases also need to be treated.
In addition to high rates of case-detection and cure, the timely identification of resistant strains can prevent the occurrence of MDR-TB,1 focusing on improved and quality-controlled bacteriology with universal drug susceptibility testing (DST), quality treatment,1 removal of healthcare access barriers, and proper monitoring and evaluation.1 The International Standards for Tuberculosis Care and its regional adaptations further underline this patient-centered approach.6
Expand Rapid Testing and Detection of Drug Resistant TBThe End TB strategy calls for early diagnosis of TB and universal DST.
Drug-resistance can be detected using phenotypic drug susceptibility testing on solid culture media (Lowenstein–Jensen; Middlebrook 7H10/11) or using liquid-based culture techniques, such as BACTEC® (BD Diagnostics, Sparks, MD, USA), MGIT® (BD Diagnostics) and BacT/ALERT® (bioMerieux SA, Marcy l’Etoile, France).
A simple, economic, rapid, point-of-care test to diagnose active TB in different populations (HIV-infected adults and children) while detecting resistance to anti-TB drugs is needed.7 Xpert MTB/RIF (Cepheid, Sunnyvale, California, USA) is therefore recommended by the WHO as the initial diagnostic test for TB and MDR-TB. It is performed in a fully automated closed system (preventing contamination), and can be used by operators with minimal expertise at the peripheral level, producing results in about 2h.1
Rifampicin-resistance is considered a reliable proxy of MDR-TB, as the prevalence of strains with rifampicin mono-resistance is low, and their clinical management requires second-line drugs.8
Recently, a new Xpert MTB/RIF Ultra assay has been developed (new sample processing cartridge, probes and optimized cartridge fluidics and PCR cycling), with the same sensitivity as liquid culture and high specificity.1,7 The small, portable Xpert Omni is expected to be launched shortly.1,7
Line probe assays (LPAs), which are used on culture isolates or fresh, microscopy-positive samples, have been recently endorsed by WHO1,7 following the Hain Version 1 test endorsement in 2008.
Both the GenoType® MTBDRplus assay, Hain Lifescience (Hain Version 2 assay) and the Nipro assay (Nipro Corporation, Japan) identify M. tuberculosis complex and detect rifampicin- and isoniazid-conferring mutations; in addition, the latter is also able to identify some common non-tubercular mycobacteria (M. avium, M. intracellulare and M. kansasii).1 Automated liquid culture systems are recommended as the ‘gold standard’ for second-line DST, allowing identification of XDR-TB in 4–9 weeks.1,7
Tests for the rapid identification of resistance to the main second-line TB drugs have also been developed (Hain Lifescience GenoType MTBDRsl). These assays can rapidly detect genetic mutations associated with resistance to fluoroquinolones, aminoglycosides (kanamycin, amikacin), cyclic peptides (capreomycin), ethambutol, and streptomycin.1,7
Provide Immediate Access to Effective Treatment and Proper CareAt present, only 1 in every 3 patients has access to adequate treatment; therapeutic success is low and the rate of treatment failure and death is high.1,2,8
The recently approved anti-TB drugs, bedaquiline and delamanid, improve bacteriological conversion and treatment outcomes when added to a background regimen designed according to WHO recommendations.1,9,10 Evidence of co-administration of these drugs is anecdotal11 and far too limited to recommend this approach.1,7,9
Other repurposed drugs have recently been studied, including linezolid12 and carbapenems13 (more recently ertapenem) and clofazimine1; there is less evidence to recommend clarithromycin and amoxicillin-clavulanate.13 A promising new regimen based on pretomanid (PA-824 – an analog of delamanid), associated with moxifloxacin and pyrazinamide is currently being tested in phase IIb trials in drug-susceptible and MDR-TB during the first 8 weeks of treatment.1,7
Several trials are currently studying possible combinations of various anti-TB drugs (STREAM phase 2 trial, TB-PRACTECAL study, NCT02333799 study on bedaquiline, pretomanid and linezolid, MDR-END study, PaMZ trial, and others). More information on these is available at https://clinicaltrials.gov.)
Moreover, an analog of linezolid, sutezolid, has shown promising efficacy and tolerability.1,7
Prevent Transmission Through Infection ControlThe WHO Policy on Infection Control1,4,14 clearly underlines the importance of effective infection control measures in clinical facilities that treat TB and M/XDR-TB patients.
The strategy includes managerial activities, together with administrative and environmental controls.1,14 Evidence exists that proper implementation of this strategy is lacking in several settings, including European Union countries.2,14 Some of the most interesting experiences in this regard include the efforts made in South Africa to reduce unnecessary hospitalizations and shorten hospital stays to reduce the risk of transmission to patients, visitors and staff. A comprehensive approach to infection control must include a paradigm shift from in-patient to out-patient care, as clearly recommended by WHO.1,14,15
Increase Political Commitment and FundingPoverty is known to increase TB occurrence, TB mortality rates, and Mycobacterium tuberculosis transmission.1,3 Although diagnosing and treating MDR-/XDR-TB can be considered expensive (even in affluent countries), the use of new drugs may be cost-effective.
The prevention and control MDR-TB is based on the correct use of new diagnostic techniques and drugs1,5–8 in combination with the core interventions described above.
Efforts to eliminate TB have recently focussed on the diagnosis and treatment of latent TB infection (LTBI) and TB control in risk groups (displaced populations).1 Both interferon-gamma release assays (IGRAs) or Mantoux tuberculin skin test (TST) are recommended to diagnose LTBI in high risk and vulnerable groups, while new regimens containing rifampicin and rifapentine are currently recommended, being particularly useful in isoniazid-resistant cases.
In some high-income countries, the highest proportion of TB cases are found among migrants and refugees, and these populations are the main source for new cases among nationals.1 After arriving in a new country, those vulnerable groups should be able to access TB services freely, and prompt, top-quality management of TB and LTBI should be guaranteed.
In order to reach TB elimination targets, clinician have the moral duty to correctly manage both drug-susceptible and MDR-TB.
FundingNo funding source.
Conflict of InterestsAll authors declare no competing interests.
This article was developed within the ALAT/ERS Collaborative SinTB project.
- Clinical characteristics and 2-year outcomes of chronic obstructive pulmonary disease patients with high blood eosinophil counts: a population-based prospective cohort study in China
- Hypersensitivity Pneumonitis-like Histological Findings Secondary to SARS-COV-2 Pneumonia
- Determinants of COVID-19 Hospitalization Costs in a Referral Hospital for Respiratory Diseases
- Multidisciplinary Consensus on the Management of Non-Invasive Respiratory Support in the COVID-19 Patient
articles




www.publicationethics.org.




Archivos de Bronconeumología follows the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals