


Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome is characterized by congenital agenesis of the uterus and vagina in women with normal ovaries, phenotype and karyotype.1,3 The associated lung malformations described are practically anecdotal.1–4 We report a case of associated partial anomalous pulmonary venous drainage.
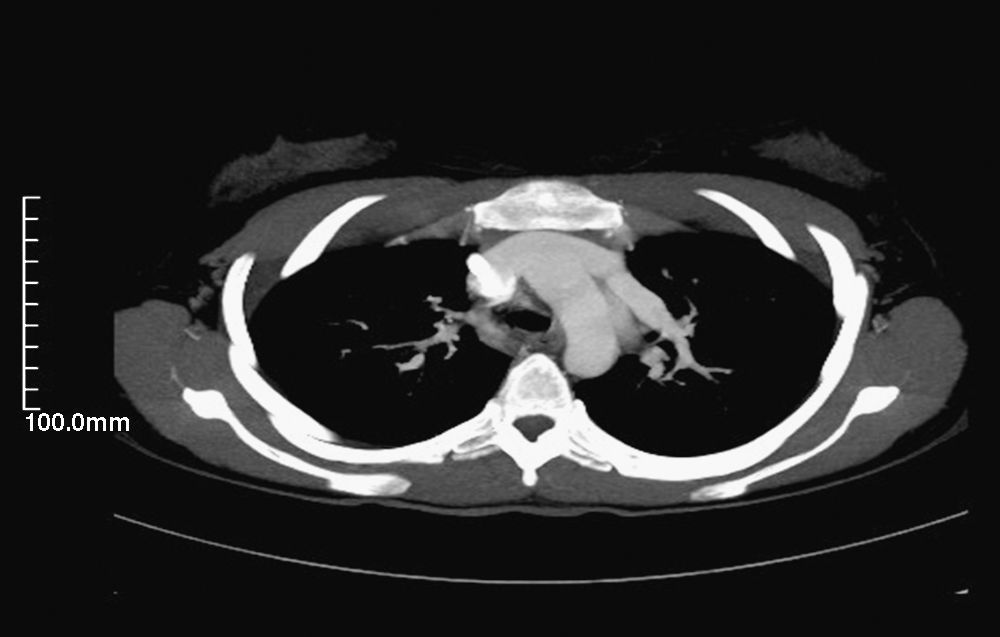
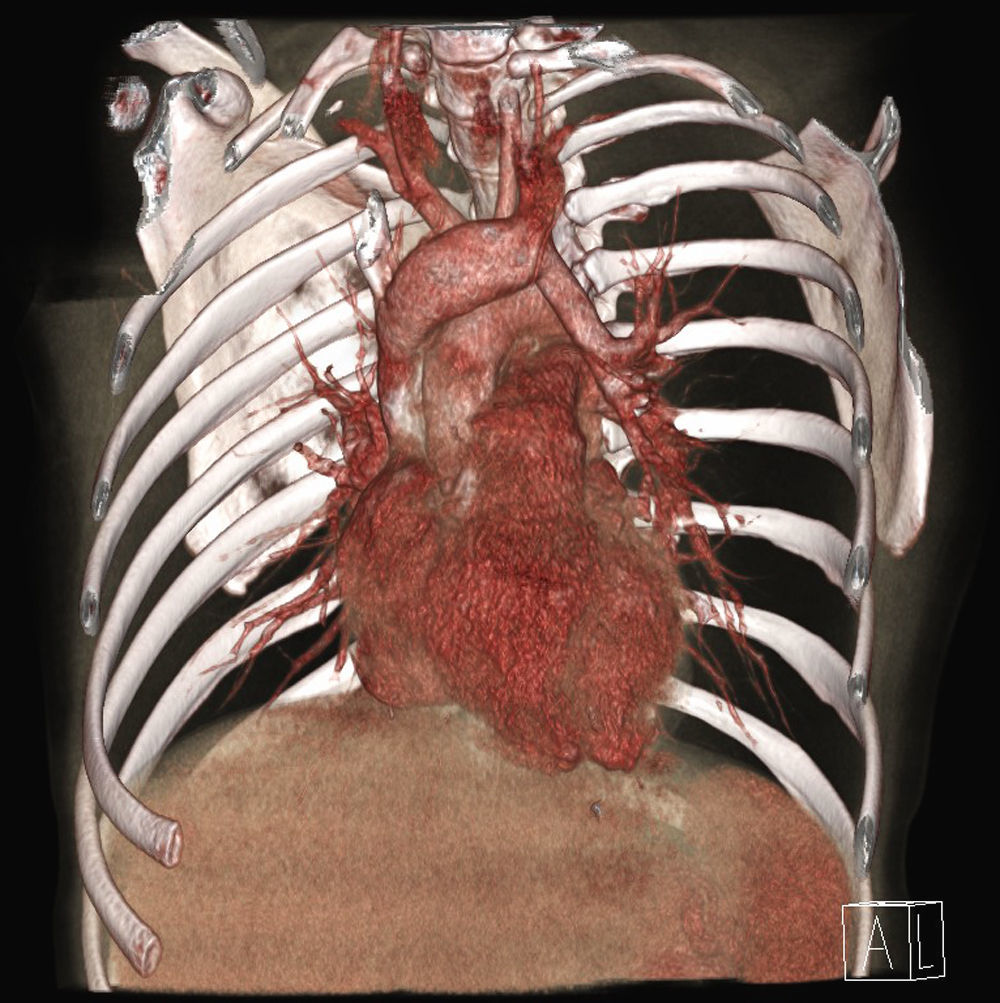
The patient is a 19-year-old woman with MRKH, who referred frequent colds and presented low-grade fever, purulent expectoration and dyspnea with minimal exertion. Physical examination was normal, except for mild tachypnea and bibasilar inspiratory rales. The work-up presented leukocytosis with neutrophilia and the arterial blood gas showed pCO2 39 and pO2 57. Chest radiograph and electrocardiogram were normal. Thoracic computed tomography (CT) and magnetic resonance imaging (MRI) revealed partial anomalous pulmonary venous drainage: the vein of the upper left lobe was draining into the innominate vein through the vertical vein (Figs. 1 and 2). Transthoracic echocardiogram with contrast ruled out intracardiac communications as well as overload of the right cavities.


MRKH is a rare malformation (incidence 1/4000 living newborns) characterized by congenital agenesis of the uterus and vagina in women with normal ovaries, secondary sex characteristics and karyotype.1–4 The etiopathogeny lies in a lack of development of the Müllerian ducts, with the consequent alteration in the structures derived from them.1 The diagnosis is based on primary amenorrhea and the inability to allow for vaginal penetration, confirmed by ultrasound and MRI.1,4 It is divided into two types: typical or I (agenesis of the uterus and vagina) and atypical or II, associated with other malformations (renal, skeletal, digital and cardiac, as well as deafness).1–4 The associated pulmonary malformations that have been published are practically anecdotal, including a case of pulmonary hypoplasia4 and a case of total anomalous pulmonary venous drainage.3 We describe a case of partial anomalous pulmonary venous drainage where the vein of the upper left lobe drains into the innominate vein through the vertical vein. Anomalous pulmonary venous drainage is produced when the pulmonary venous blood from one or more veins flows directly into the right auricle or in the systemic veins. It may be total (4 anomalous veins) or partial (1–3 anomalous veins). In both types, a left-to-right extracardiac shunt is produced, causing an increase in bloodflow with the consequent overload in the right auricle and ventricle, as well as in the pulmonary artery and veins. This hyperflow can cause heart failure and pulmonary hypertension. The hemodynamic overload depends on the number of veins with anomalous connection, the location of the drainage and whether it is associated with intraauricular communication. Thus, the patients can be asymptomatic, present frequent colds—as in our case—or present heart failure and pulmonary hypertension. The anomalous vein on occasion can be seen on simple radiography, confirming the diagnosis by CT and MRI, and resorting to cardiac catheterization when given the suspicion of pulmonary hypertension.
Please cite this article as: Zorrilla-Lorenzo V, et al. Drenaje venoso pulmonar anómalo parcial y síndrome de Mayer-Rokitansky-Kuster-Hauser. Arch Bronconeumol. 2011;47:473–4.







