


Tracheal diverticula are a rare affectation. They are usually diagnosed as an incidental finding by thoracic computed tomography (CT) or bronchoscopy. Although it is a very rare cause of difficulty for intubation (there are only three reported cases worldwide), its diagnosis should be made or its presence ruled out in order to avoid major complications.
We present the case of a 77-year-old woman with a large acquired tracheal diverticulum who presented many difficulties for orotracheal intubation and hemoptysis.
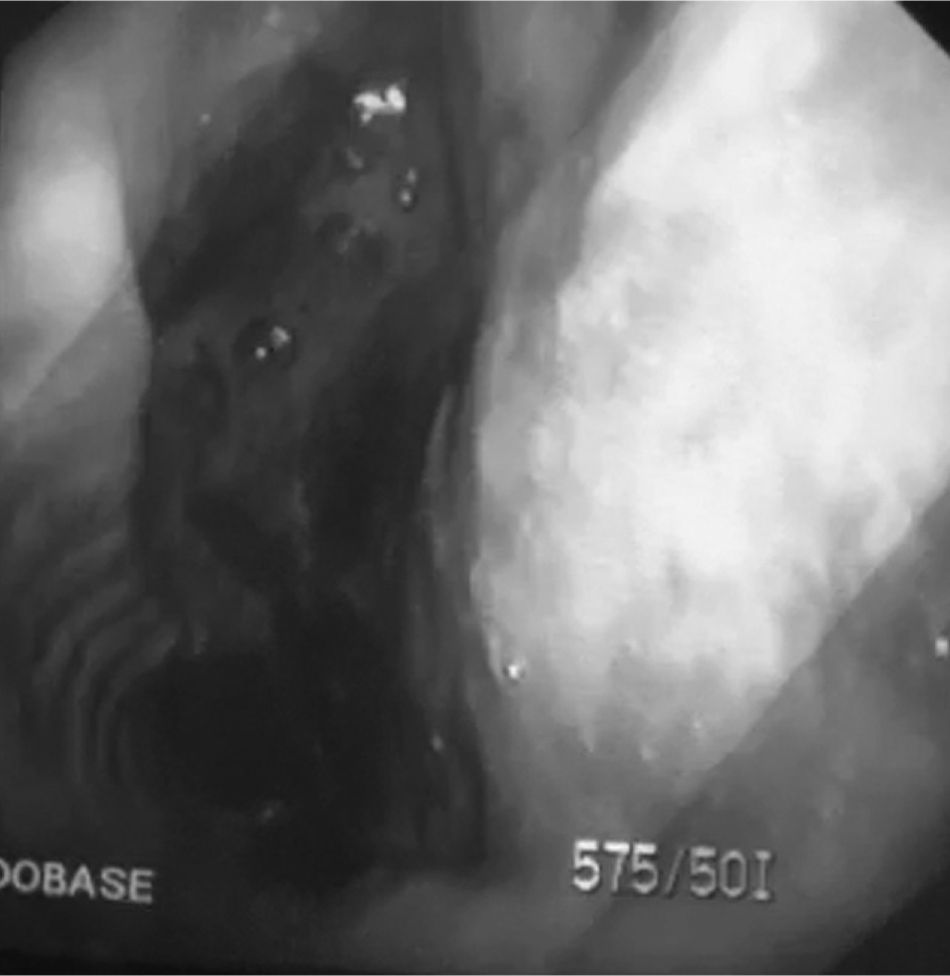
The patient presented myocardial infarction with cardiorespiratory arrest; cardiopulmonary resuscitation was begun and orotracheal intubation was very difficult. Once hospitalized, a mild hemorrhage was seen through the endotracheal tube. Thus, bronchoscopy was performed, at which time we observed what was interpreted as an interruption on the right lateral face of the trachea covered with clots. We contacted the Thoracic Surgery team that was on call and chest CT was ordered, upon which we observed that the distal third of the trachea was hyperinflated. There was also irregular morphology of the right wall of the trachea at this level, which was compatible with laceration. Given the findings of the CT but the lack of clinical signs of tracheal rupture, a new bronchoscopy was performed (Fig. 1) with the patient in a stable respiratory and hemodynamic state. During this exploration, in the distal third we observed an image of a large sack of tracheal mucosa with no apparent rupture. The lesion was diagnosed as tracheal diverticulum and the patient was extubated without incident. The patient was discharged and continued to be asymptomatic at the follow-up visit two months later.

There are two different types of tracheal diverticula: congenital and acquired. Congenital tracheal diverticula are present as sac formations that are connected with the trachea through a narrow isthmus, which on occasion may not be seen. They have the same histologic characteristics as the trachea.1 They are usually small and may be accompanied by other malformations of the tracheobronchial tree. Those that are acquired, as we believe is the case of the patient that we present, consist of a herniation of the mucosa through a weak spot in the tracheal wall due to an increase in the endoluminal pressure.2 Histologically, they have a thin wall that is basically composed of respiratory epithelium and do not present a cartilaginous component. Acquired tracheal diverticula are larger and present a more extensive connection with the trachea than congenital diverticula.
Both in congenital as well as in acquired diverticula, the most frequent location is the right posterolateral tracheal wall, as in the case that we present. It has been proposed that the cause of this difference is the relative weakness presented by the right paratracheal region compared with the left due to the presence of the aortic arch and the esophagus, which provide structural support to the tracheal wall.3
For the diagnosis, the test of choice is cervical-thoracic CT although in cases such as this that we have presented, in which the patient was intubated, this imaging technique may not define a diagnosis as it can be interpreted as tracheal rupture. In any case, the definitive diagnosis must be done with bronchoscopy,4 which provides a vision of the tracheal communication. In acquired diverticula, this communication is large in caliber; therefore, bronchoscopy gives a clear image. As for the differential diagnosis, in our case we considered a post-intubation tracheal laceration given the difficulty of the intubation and the hemorrhage through the tube. This pathology should be considered in cases of difficult intubation as, although rare, several cases with this problem for intubation have been described.5,6
The treatment of this pathology in cases of not being symptomatic is generally conservative as it is a benign pathology. In our case, the patient did not receive any treatment given the absence of symptoms. In cases in which there are symptoms, surgical treatment of the lesion should be performed, including extirpation and reinforcement of the tracheal wall.
Please cite this article as: Carmona Soto P, et al. Divertículo traqueal adquirido como causa de intubación orotraqueal complicada. Arch Bronconeumol. 2011;48:64–5.







