


A 29-year-old patient presented to our hospital with fever and left upper chest swelling. A chest radiograph showed a left pleural effusion and an ill-defined focal lesion in the left superior hemithorax (Fig. 1A). A thoracic CT showed an extrapleural fluid collection extending from the left sternochondral joint of the first rib towards the left upper lobe as well as small fluid rim-enhancing collections involving the left pectoralis muscles, consistent with soft-tissue abscesses (Fig. 1B). There was also a loculated posterior ipsilateral pleural effusion (Fig. 1C). The diagnosis of a septic sternochondral arthritis of the first rib complicated with an ipsilateral pleural empyema was made. It was decided to insert pigtail catheters both into the extrapleural fluid collection and into the left pleural space under CT guidance in a single procedure (Fig. 1D and E). The procedure was uneventful and demonstrated Staphylococcus aureus, both in the extrapleural fluid collection and in the left pleural effusion. The patient responded well to antibiotic therapy, and surgical debridement was not deemed necessary (Fig. 1F and G).
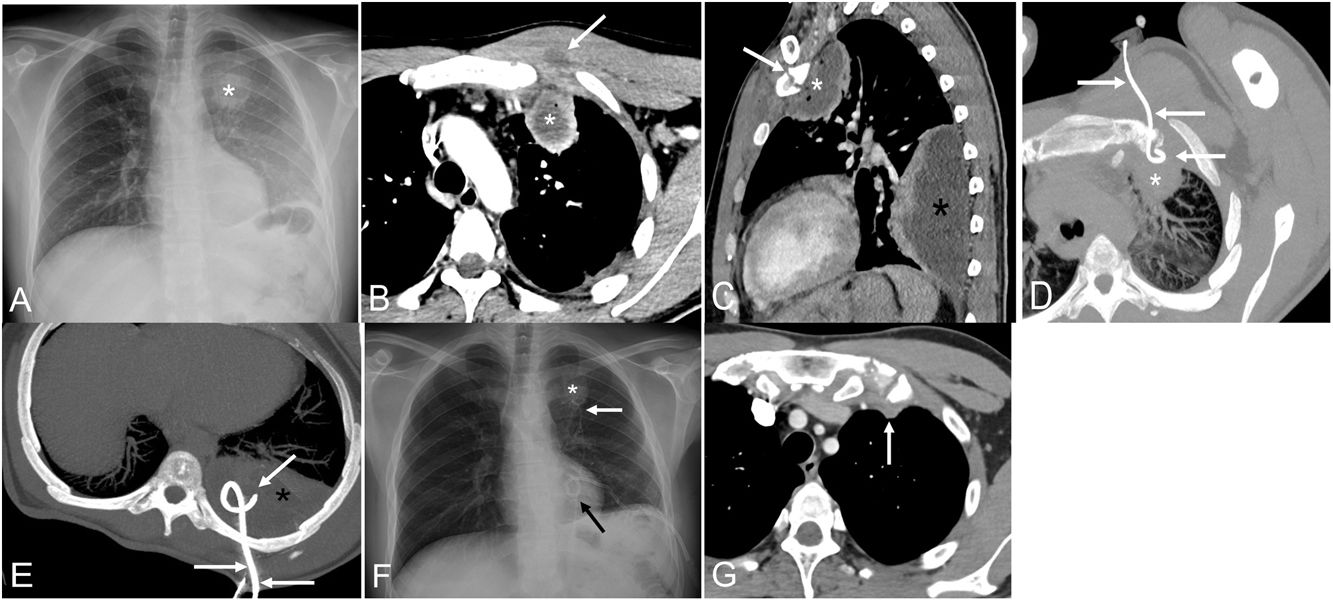
 Chest radiograph (posteroanterior view) shows an ill-defined lesion projected over the sternochondral joint of the first left rib (asterisk). Note the increased density of the left hemithorax due to an ipsilateral pleural effusion. (B) Axial thoracic CT image (mediastinal window) shows an extrapleural fluid collection (asterisk) and demonstrates a small low-attenuation lesion in the left pectoralis major muscle (arrow). (C) Sagittal thoracic CT image (mediastinal window) better shows the extrapleural fluid collection (white asterisk) originating in the first sternochondral joint (arrow) and a large loculated pleural effusion (black asterisk). (D) Axial thoracic maximum intensity projection (MIP) CT image shows a pigtail catheter (arrows) within the extrapleural fluid collection (asterisk). (E) Axial thoracic MIP image shows another pigtail catheter (arrows) within the left pleural effusion. (F) Chest radiograph (posteroanterior view) obtained 1 week after the insertion of the pigtail catheters (arrows) shows marked improvement. Note the reduction in size of the extrapleural lesion in the left upper hemithorax (asterisk). (G) Axial thoracic CT image (mediastinal window) performed 8 weeks after the insertion of the pigtail catheter shows complete resolution of the extrapleural collection and minimal residual thickening of the soft tissues surrounding the first sternochondral joint (arrow).")
(A) Chest radiograph (posteroanterior view) shows an ill-defined lesion projected over the sternochondral joint of the first left rib (asterisk). Note the increased density of the left hemithorax due to an ipsilateral pleural effusion. (B) Axial thoracic CT image (mediastinal window) shows an extrapleural fluid collection (asterisk) and demonstrates a small low-attenuation lesion in the left pectoralis major muscle (arrow). (C) Sagittal thoracic CT image (mediastinal window) better shows the extrapleural fluid collection (white asterisk) originating in the first sternochondral joint (arrow) and a large loculated pleural effusion (black asterisk). (D) Axial thoracic maximum intensity projection (MIP) CT image shows a pigtail catheter (arrows) within the extrapleural fluid collection (asterisk). (E) Axial thoracic MIP image shows another pigtail catheter (arrows) within the left pleural effusion. (F) Chest radiograph (posteroanterior view) obtained 1 week after the insertion of the pigtail catheters (arrows) shows marked improvement. Note the reduction in size of the extrapleural lesion in the left upper hemithorax (asterisk). (G) Axial thoracic CT image (mediastinal window) performed 8 weeks after the insertion of the pigtail catheter shows complete resolution of the extrapleural collection and minimal residual thickening of the soft tissues surrounding the first sternochondral joint (arrow).
Septic isolated sternochondral arthritis of the first rib is extremely rare and very few cases have been published.1 To our knowledge most of sternochondral arthritis of the first rib occur as part of a more extensive infection involving both the sternoclavicular and the first sternochondral joints, and the majority of reported cases require intravenous therapy and surgical debridement in order to control the infection.2 Our patient developed a pleural empyema as a complication of the septic arthritis. We believe that prompt percutaneous drainage of both the extrapleural collection adjacent to the first sternochondral joint and the pleural empyema (along with intravenous antibiotics) allowed a nonsurgical management of this unusual infection.
Conflict of InterestsThe authors state that they have no conflict of interests.







