


High-grade pulmonary Non-Hodgkin B-cell lymphoma is rare and classics manifestations are systemic symptoms and post-obstructive pneumonia.1 Radiological findings typically describe a single pulmonary mass associated with mediastinal or hilar adenopathies and endobronchial involvement is unusual.1,2 Tissues samples show a solid neoplastic tissue, consisting of medium to large sized cells with marked nuclear pleomorphism. Lymphomatous cells express B-lineage markers (CD20, CD19, PAX5). Small cell lung cancer is associated with tobacco consumption and usually presents as a hilar mass associated with bulky hilum and mediastinal lymph nodes involvement.3 Endobronchial involvement is rare. Neoplastic tissue shows a solid growth, small round/oval cells with high nuclear to cytoplasmic ratio. Neoplastic cells show a “dot-like” expression of cytokeratins and expression of neuroendocrine markers (Chromogranin-A, synaptophysin, CD56).3
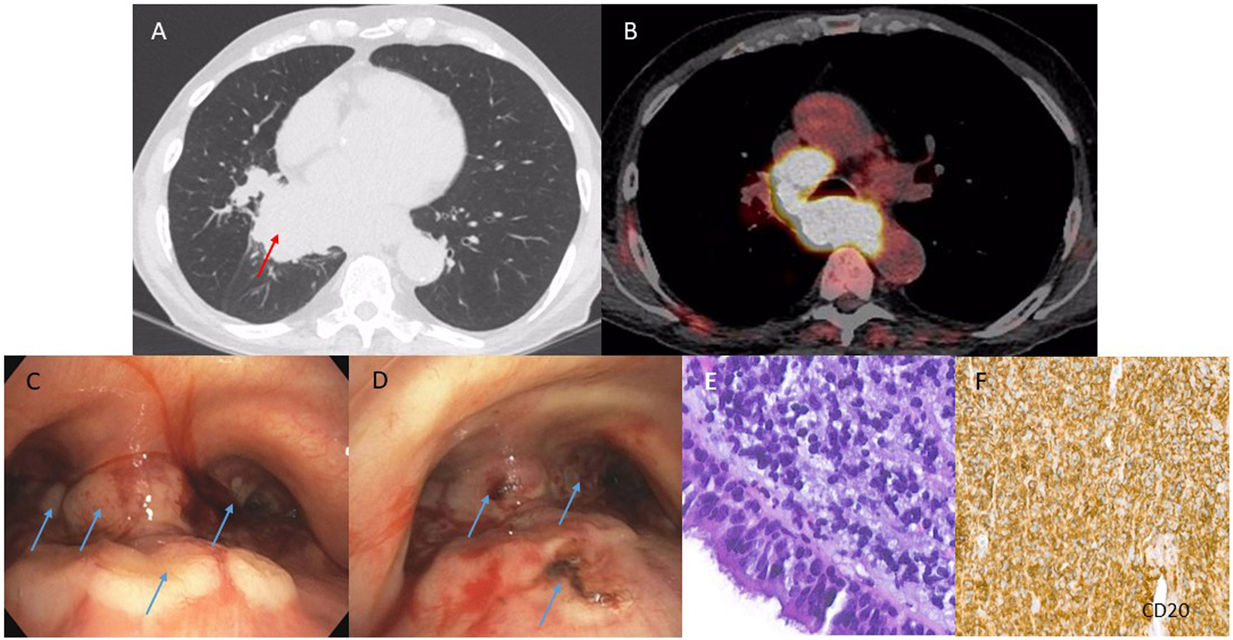
A 82-years old former smoker patient was assessed for progressive asthenia and non-severe recurrent haemoptysis. The Computed Tomography-scan showed a right lower lobe sub-hilar mass (Fig. 1A) associated with bulky mediastinal adenopathies (Fig. 1B). The bronchoscopy documented the presence of well-vascularized endoluminal implants causing bleeding and treated by laser Argon-Beamer (Fig. 1C, D). Both samplings guided by endobronchial ultrasound at lymph nodes stations 7/4R and endobronchial targeted biopsies were consistent with diffuse large B-cell lymphoma (Fig. 1E, F).
 and mediastinal enlarged lymph node stations (7 and 4R) on axial view on Positron Emission Tomography CT-scan showing a high avidity for fluorodeoxyglucose-F18 tracer (B, color). Endobronchial implants located at the distal pars membranacea of the trachea, main carina and main bronchi (C, blue arrows) treated by laser Argon-Beamer (D, blue arrows). Endobronchial samplings with solid growth neoplasm infiltrating the bronchial mucosa, made up of medium-sized cells, with moderately pleomorphic and hyperchromatic nuclei (E, hematoxylin–eosin staining 400×). Neoplastic cells express B-lineage marker CD20 (F). The diagnosis of B-cell lymphoma was also confirmed by molecular analysis.")
Mass on axial view on pulmonary windowing (A, red arrow) and mediastinal enlarged lymph node stations (7 and 4R) on axial view on Positron Emission Tomography CT-scan showing a high avidity for fluorodeoxyglucose-F18 tracer (B, color). Endobronchial implants located at the distal pars membranacea of the trachea, main carina and main bronchi (C, blue arrows) treated by laser Argon-Beamer (D, blue arrows). Endobronchial samplings with solid growth neoplasm infiltrating the bronchial mucosa, made up of medium-sized cells, with moderately pleomorphic and hyperchromatic nuclei (E, hematoxylin–eosin staining 400×). Neoplastic cells express B-lineage marker CD20 (F). The diagnosis of B-cell lymphoma was also confirmed by molecular analysis.







