
Lung cancer (LC) is a serious health problem due to its high incidence and mortality. Surgery is the most effective therapeutic strategy in this type of tumor, but in recent years new drugs are being investigated that target specific components of the tumor cells, improving survival in patients with advanced disease and relapse. We present a review of individualized treatments in LC, particularly therapies that inhibit epidermal growth factor receptor (EGFR), vascular endothelial growth factor (VEGF) and anaplastic lymphoma kinase (ALK).
El cáncer de pulmón (CP) es un grave problema sanitario debido a su elevada incidencia y mortalidad. La cirugía es la más eficaz de las estrategias terapéuticas en este tipo de tumor, pero en los últimos años se están investigando nuevos fármacos contra componentes diana específicos de las células tumorales, que mejoran la supervivencia en pacientes con enfermedad avanzada y recurrencias. Presentamos una revisión de los tratamientos individualizados en el CP, en particular las terapias inhibidoras del receptor de crecimiento epidérmico (EGFR), del factor de crecimiento endotelial vascular (VEGF) y de la kinasa del linfoma anaplásico (ALK).
LC is the main cause of death by cancer in the world,1,2 causing 1.3 million deaths per year (29% of cancer deaths).3 More than 80% of LC are non-small-cell lung carcinoma (NSCLC), which include various differentiated histological types, such as adenocarcinoma (the most frequent form overall, representing 38% of cases), squamous or epidermoid carcinoma and large-cell carcinoma, among others.4 Long-term survival is poor and 5-year survival rates ranges between 7% and 15%.1,2 This is due to the fact that most patients are diagnosed in early stages, where the option of surgical treatment (which is to date the most effective therapeutic strategy) no longer exists.5–8
In recent years, numerous molecular alterations have been researched (mutations, genic amplifications) that are responsible for tumor survival, and which therefore influence the vital prognosis of patients. Treatments that have an effect on these alterations are so-called target or individualized therapies, which are based on recognizing common molecular or clinical alterations and may provide hope for improving survival in non-surgical stages.
Because of its therapeutic implications, one of the most commonly studied mediators is EGFR, which plays a role in cell growth, proliferation and motility.9 EGFR inhibitor drugs (anti-EGFR) have been developed, such as erlotinib and gefitinib, which have been shown to improve survival in patients with advanced and recurrent disease.
Another molecule being researched is VEGF, which is involved in the tumor angiogenesis process. High tumor or serum levels have been related with advanced stages and poor survival.10 Bevacizumab is a humanized monoclonal antibody that binds with and neutralizes VEGF.11
Recently, a new drug called crizotinib has been approved for use in NSCLC. It inhibits ALK, an oncogene that is positive in around 5%–13% of patients with NSCLC, and its inhibition has a beneficial effect on survival.12
In this article, we will review the current scientific evidence on these treatments.
EGFR InhibitorsEGFR is a transmembrane glycoprotein with tyrosine kinase (TK) activity that is coded by a gene located in the 7p12 chromosome. It is one of the 4 members of the TK human epidermal receptor (HER) family.13 EGFR plays a considerable role in carcinogenesis and its overexpression has been related with advanced disease and poor prognosis.14 Mutations that affect the TK domain have only been described in NSCLC, and the most frequent are found in exons 19 and 21.15,16 These mutations are determined in tumor tissue embedded in paraffin, and they are especially associated with the adenocarcinoma subtype, especially bronchioloalveolar, and Asian women and non-smokers.17,18 Patients with these mutations have a high probability of responding to anti-EGFR therapies. Currently, there has been more experience with erlotinib and gefitinib, both of which reversibly inhibit the catalytic activity of the receptor, interrupt the transduction of the growth signal and produce an anti-tumor effect. They have been most closely associated with the partial response or clinical improvement of patients with EGFR gene mutations.19
Shepherd et al.20 demonstrated that erlotinib, used as a single agent, prolonged survival in patients with NSCLC after first- or second-line chemotherapy (CTx) (P=.001). The one-year survival improved from 21% to 31%, above all in never-smoker patients. This is the first study that confirmed that an anti-EGFR prolonged survival after first- or second-line CTx, and its clinical use was approved in the United States in 2004. However, in the IRESSA Survival Evaluation in Lung Cancer (ISEL) study,21 gefitinib in patients with advanced NSCLC did not improve survival when compared to placebo (P=.08). Nonetheless, survival in the treatment group was significantly longer in never-smokers and in the Asian population.
In a prospective study of the Spanish Lung Cancer Group22 that included 2105 patients, the EGFR mutation was present in 16.6% and 217 patients received treatment with erlotinib, which was the first line of treatment in 113. In these patients, the mean survival time was 14 months and the average global survival was 27 months. This cohort study demonstrated that large-scale screening of patients for EGFR mutations and treatment with anti-EGFR was feasible. The results of these studies also support the concept that, in a particular subgroup of patients, the first line of treatment with anti-EGFR drugs may be the most effective option.
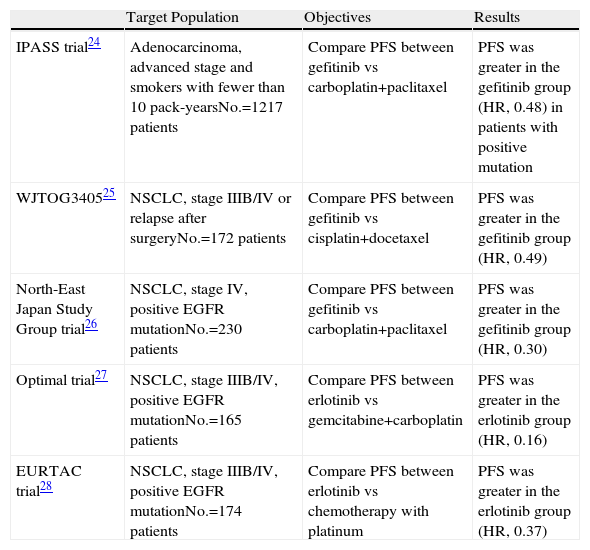
In the recent Iressa Pan-Asia Study (IPASS),23 first-line gefitinib was compared with carboplatin/paclitaxel in 1217 patients with advanced NSCLC. Eligible patients were either non-smokers or ex-smokers with limited consumption who had histology for adenocarcinoma. The frequency for EGFR mutations was 59.7%. The analysis demonstrated that patients with EGFR mutations had a higher average survival time in the gefitinib subgroup compared with the standard CTx subgroup (HR, 0.48; P<.001). This is an argument in favor of the fact that mutation tests should become a mandatory practice when NSCLC is diagnosed, at least for patients with adenocarcinoma, never-smokers or smokers with limited consumption. These patients should be treated with anti-EGFR drugs if their tumors express the mutation, given the demonstrated benefit. In any event, it is important to observe that the IPASS study was done in Asia and that the EGFR mutations are less frequent in Caucasians (40% and 10%, respectively). Table 1 summarizes the results of the main studies in phase III with erlotinib and gefitinib.23–28
Main Studies in Phase III With Anti-EGFR Drugs.
| Target Population | Objectives | Results | |
| IPASS trial24 | Adenocarcinoma, advanced stage and smokers with fewer than 10 pack-yearsNo.=1217 patients | Compare PFS between gefitinib vs carboplatin+paclitaxel | PFS was greater in the gefitinib group (HR, 0.48) in patients with positive mutation |
| WJTOG340525 | NSCLC, stage IIIB/IV or relapse after surgeryNo.=172 patients | Compare PFS between gefitinib vs cisplatin+docetaxel | PFS was greater in the gefitinib group (HR, 0.49) |
| North-East Japan Study Group trial26 | NSCLC, stage IV, positive EGFR mutationNo.=230 patients | Compare PFS between gefitinib vs carboplatin+paclitaxel | PFS was greater in the gefitinib group (HR, 0.30) |
| Optimal trial27 | NSCLC, stage IIIB/IV, positive EGFR mutationNo.=165 patients | Compare PFS between erlotinib vs gemcitabine+carboplatin | PFS was greater in the erlotinib group (HR, 0.16) |
| EURTAC trial28 | NSCLC, stage IIIB/IV, positive EGFR mutationNo.=174 patients | Compare PFS between erlotinib vs chemotherapy with platinum | PFS was greater in the erlotinib group (HR, 0.37) |
NSCLC: non-small-cell lung cancer; PFS: progression-free survival; HR: hazard ratio.
On the other hand, a meta-analysis of 4 studies in phase III comparing gefitinib with standard QT concludes that there are no differences in mean survival between the 2 groups, but in the group of patients treated with gefitinib fewer side effects and a better quality of life are observed than in those who received standard CTx.29
In our setting, the mutation of the EGFR gene is observed in approximately 15% of NSCLC.30,31 Around 75% of the cases with this mutation respond to treatment with erlotinib/gefitinib, while in the non-mutated cases only 10% respond.32 However, almost all the patients who respond initially wind up having a progression of the disease. The causes of this acquired resistance to anti-EGFR drugs are not completely understood, but there seem to be different mechanisms involved, such as secondary EGFR mutations or an amplification of the MET oncogene.33,34
VEGF InhibitorsThe VEGF gene is located in the 6p21.3 chromosome. It is a key mediator in angiogenesis,10 as it is the most powerful angiogenic factor that we know of.11 An increased VEGF expression in either the tumor or serum has been associated with advanced-stage tumors, and their levels are significantly higher in adenocarcinoma than in squamous carcinoma.35 The VEGF family is made up of different proteins, called VEGF-A, VEGF-B, VEGF-C, VEGF-D and PIGF (placental growth factor).36
The effects of VEGF include: increased endothelial cell mitosis, control of vascular permeability and increased survival of the vascular endothelium, etc.37 VEGF carry out these functions by bonding with their receptors (VEGFR), which are found in the endothelial cells. There are three types of receptors: VEGFR-1, VEGFR-2 and VEGFR-3, all with TK activity.38
Carrillo et al.39 researched VEGF and their receptors in patients with NSCLC and their correlation with prognosis. The patients with moderate/high VEGF-C, VEGFR-1 and VEGFR-2 expression had poorer survival, while survival was better in patients with moderate/high expression of VEGF-D and VEGFR-3. In the multivariate analysis, stage and VEGF-D and VEGFR-1 expression were significant independent prognostic factors. On the other hand, a meta-analysis of 20 studies by Delmotte et al.,35 demonstrated that VEGF-A expression was an unfavorable prognostic factor in patients with NSCLC. The results of these studies suggest that the expression profiles of VEGF and VEGFR may have prognostic value in NSCLC and may help identify patients that, potentially, may be good responders to anti-angiogenic therapies.
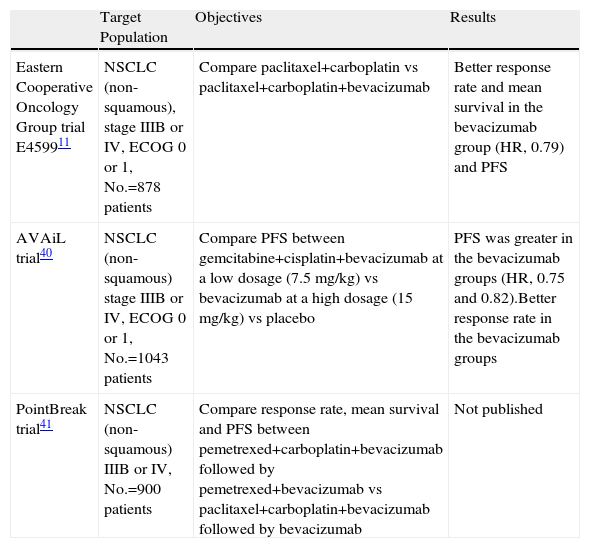
The importance of VEGF makes it an attractive target for the development of new directed therapies. Bevacizumab is a humanized monoclonal antibody that binds with and neutralizes all the VEGF-A isoforms. The efficacy and safety of bevacizumab have been evaluated in 3 studies in phase III,11,40,41 whose general characteristics can be consulted in Table 2. Briefly, treatment with bevacizumab was observed to provide a longer mean survival and a tendency towards increasing survival. There was, however, an observed increased risk for bleeding, especially in centrally located tumors that are close to large vessels and with squamous carcinoma histology.
Studies in Phase III With Bevacizumab.
| Target Population | Objectives | Results | |
| Eastern Cooperative Oncology Group trial E459911 | NSCLC (non-squamous), stage IIIB or IV, ECOG 0 or 1, No.=878 patients | Compare paclitaxel+carboplatin vs paclitaxel+carboplatin+bevacizumab | Better response rate and mean survival in the bevacizumab group (HR, 0.79) and PFS |
| AVAiL trial40 | NSCLC (non-squamous) stage IIIB or IV, ECOG 0 or 1, No.=1043 patients | Compare PFS between gemcitabine+cisplatin+bevacizumab at a low dosage (7.5mg/kg) vs bevacizumab at a high dosage (15mg/kg) vs placebo | PFS was greater in the bevacizumab groups (HR, 0.75 and 0.82).Better response rate in the bevacizumab groups |
| PointBreak trial41 | NSCLC (non-squamous) IIIB or IV, No.=900 patients | Compare response rate, mean survival and PFS between pemetrexed+carboplatin+bevacizumab followed by pemetrexed+bevacizumab vs paclitaxel+carboplatin+bevacizumab followed by bevacizumab | Not published |
NSCLC: non-small-cell lung cancer; PFS: progression-free survival; HR: hazard ratio.
The dual inhibition of EGFR and VEGF is currently being researched. There are 2 strategies: the first is to combine 2 agents with specific anti-target pathways, like erlotinib and bevacizumab,42 and the other is the use of an agent with dual activity, like vandetanib, a small molecule with activity against VEGFR-2, -3, and anti-EGFR.43 Recently, results have been published from a clinical assay including 1240 patients with NSCLC in stages IIIB and IV who had already received at least one first-line CTx. The patients were randomized into 2 treatment groups, one receiving vandetanib and the other erlotinib, and no differences were observed in survival between the two groups (P=.83).44
ALK InhibitorsIn a subgroup of patients with NSCLC, their tumors present a genetic mutation that consists of the rupture in the EML4 (echinoderm microtubule-associated protein-like 4) and ALK genes, and a later fusion of the two genes in the opposite direction.45 The final result is the EML4-ALK oncogene, which inhibits apoptosis and favors tumor proliferation.45 This oncogene is present in a relatively low percentage of patients with NSCLC (around 5%).46–48 It has been seen that it is more frequent in young patients, non-smokers or smokers with low accumulated tobacco consumption, and the adenocarcinoma type.46 In this type of population, the frequency of EML4-ALK can reach 13%.48
In August 2011, a new drug was approved for sale in order to treat advanced-stage NSCLC, called crizotinib, which inhibits EML4-ALK.49 Its efficacy was demonstrated in 2 multicenter studies at a dosage of 250mg/twice daily, taken orally.50 In those 2 studies, in total 255 patients were included whose tumors contained the EML4-ALK oncogene, 95% of whom had metastatic disease. It was confirmed that treatment with crizotinib produced either a complete or partial response in 55% of patients, and the median response duration was between 42 and 48 weeks.50,51 Treatment with this drug was well-tolerated and the most common side effects were visual alterations, gastrointestinal problems and alterations in the hepatic profile.50
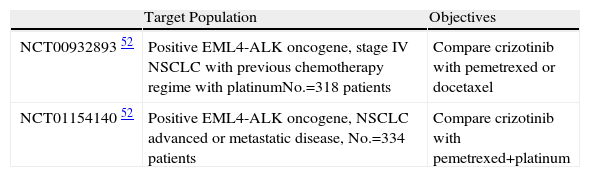
There are currently 2 studies being done in phase III about the role of crizotinib in the treatment of NSCLC.52 Their characteristics are shown in Table 3. Resistance to treatment with crizotinib has been reported after a good initial response, which has been related with mutations in the TK domain of ALK.53
Studies Underway in Phase III With Crizotinib.
| Target Population | Objectives | |
| NCT0093289352 | Positive EML4-ALK oncogene, stage IV NSCLC with previous chemotherapy regime with platinumNo.=318 patients | Compare crizotinib with pemetrexed or docetaxel |
| NCT0115414052 | Positive EML4-ALK oncogene, NSCLC advanced or metastatic disease, No.=334 patients | Compare crizotinib with pemetrexed+platinum |
Currently, other molecules are being researched for the treatment of advanced or recurring LC. An example is amrubicin, a drug that exerts its anti-tumor effect by inhibiting topoisomerase II.54 Recently, a study has been published in phase I54 in which this drug was administered to patients with NSCLC and SCLC, observing a response rate of 15.4%. Thus, in coming years, we will continue to see advances made in the treatment of LC in non-surgical stages.
ConclusionsAnti-EGFR drugs and VEGF and EML4-ALK inhibitors improve disease-free survival in certain groups of patients with advanced or recurring NSCLC, providing better tolerance and quality of life and fewer side effects than conventional CTx. Therefore, the molecular study of tumor tissue is necessary to optimize the management of LC and to attain future improvements in prognosis.
Conflict of InterestsThe authors have no conflict of interest to declare.
Please cite this article as: Parente Lamelas I, et al. Terapias dirigidas en el cáncer de pulmón: ¿una nueva esperanza? Arch Bronconeumol. 2012;48:367–71.







